The “10,000 steps” goal originated as a marketing slogan for a Japanese pedometer in 1965. While more movement is generally better, the scientific “sweet spot” for mortality benefits is actually lower and more efficient.
The Curve of Diminishing Returns
A 2019 study published in JAMA Internal Medicine tracked 16,000 older women and found that mortality rates significantly decreased as step counts increased, but only up to approximately 7,500 steps per day. Beyond this point, the health benefits began to level off.
The Minimalist Strategy
1. The 7,500 Floor: Treat 7,500 steps as your daily “Minimum Effective Dose.”
2. Intensity Spikes: 3,000 steps taken at a “brisk” pace (100 steps per minute) provide greater cardiovascular adaptations than 6,000 slow strolls.
3. The Morning light Walk: Combine your steps with early morning sunlight to anchor your circadian rhythm and improve your [Sleep Score](/sleep-calculator/).
The Epidemiology of Ambulatory Activity: Deconstructing the 10,000-Step Paradigm
The ubiquity of the 10,000-step daily goal has cemented itself within the global public health consciousness, serving as the default heuristic for wearable fitness technologies, corporate wellness programs, and consumer health algorithms. This numerical target has fundamentally shaped individual behavioral modifications and physical activity tracking on a global scale. The sheer simplicity of a round, five-figure metric provides an easily communicable goal that transcends linguistic and cultural barriers, leading to widespread adoption by major health organizations and technology manufacturers. However, the foundational origin of this metric is not rooted in rigorous, longitudinal epidemiological research, nor was it derived from randomized controlled trials analyzing mortality outcomes. Rather, the 10,000-step paradigm originated as a highly successful corporate marketing strategy deployed in mid-twentieth-century Japan.
Over the past decade, the proliferation of device-measured ambulatory data—facilitated by triaxial accelerometers in massive prospective cohort studies—has allowed public health researchers, kinesiologists, and epidemiologists to precisely map the dose-response relationship between daily step volume, stepping intensity (cadence), and long-term health outcomes. The integration of these digital tracking devices into large-scale demographic studies, such as the UK Biobank and the National Health and Nutrition Examination Survey (NHANES), has generated highly granular datasets that challenge longstanding assumptions. Current epidemiological evidence reveals a highly nuanced reality regarding human locomotion: while higher step volumes are undeniably inversely associated with all-cause mortality, cardiovascular disease, oncological incidence, and cognitive decline, the scientific “sweet spot” for optimal risk reduction is substantially lower than 10,000 steps for the vast majority of demographics. Furthermore, the point at which health benefits begin to plateau is highly dependent on an individual’s chronological age, baseline sedentary time, and preexisting cardiometabolic risk factors.
This comprehensive report provides an exhaustive synthesis of the contemporary epidemiological literature regarding ambulatory activity. By deconstructing the historical genesis of the 10,000-step myth, analyzing massive international meta-analyses concerning all-cause mortality, exploring the neurovascular and cardiometabolic consequences of variable step volumes, and evaluating the highly contentious academic debate between step volume versus step intensity, this document outlines an evidence-based, physiological framework for understanding human movement and its profound, dose-dependent impact on human longevity.
The Historical Genesis and Sociocultural Entrenchment of a Marketing Heuristic
To fully comprehend the deep entrenchment of the 10,000-step benchmark in modern medical literature and consumer behavior, it is necessary to examine the socio-cultural, economic, and commercial landscape of 1960s Japan. In the immediate aftermath of the 1964 Tokyo Olympic Games, the Japanese populace experienced a massive surge in national focus on athletic achievement, physical activity, and preventative health. The international spectacle of the Olympics catalyzed a domestic fitness boom, fostering a cultural environment highly receptive to innovations in personal health monitoring. Simultaneously, the nation was undergoing a period of rapid post-war economic expansion and technological industrialization, leading to massive urbanization, a dramatic shift toward sedentary white-collar labor, and an emerging public health concern regarding rising obesity rates and the subsequent risk of coronary heart disease.
The Creation of the Manpo-kei
Amidst this profound cultural and economic shift, a Japanese manufacturer specializing in industrial instruments and special watches, Yamasa Tokei (internationally known as Yamax), sought to capitalize on the burgeoning fitness movement. In 1965, the company developed, manufactured, and launched the world’s first commercial, wearable step-counter. This rudimentary pedometer was a smart-looking gadget designed to fit snugly onto the user’s waist, utilizing a mechanical pendulum to detect the impact of footsteps. The device was priced at ¥2,200, which was considered a slightly upmarket consumer good at the time, given that the average monthly salary of a school teacher was less than ¥40,000.
The branding of this device was a masterstroke of consumer marketing. The product was named the “Manpo-kei”. In Japanese typography, this translates literally and visually to a “10,000-step meter.” The linguistic breakdown of the product name is as follows:
- 万 (man) — 10,000
- 歩 (po) — step
- 計 (kei) — measure or meter
The selection of the number 10,000 was largely arbitrary from a rigorous epidemiological standpoint. It was chosen primarily because the Japanese character for 10,000 (万) visually resembles a human figure walking or striding forward. The branding was incredibly successful and resonated deeply with the Japanese consumer base. Much like proprietary eponyms in Western markets where brand names become interchangeable with the product itself (such as Hoover for vacuums or Jacuzzi for hot tubs), “Manpo-kei” became entirely synonymous with the pedometer itself in the Japanese lexicon. This cultural saturation occurred despite the fact that the technically accurate Japanese word for a step-counting device is hosuukei.
Dr. Yoshiro Hatano and the Caloric Expenditure Hypothesis
While the initial figure of 10,000 was undeniably a marketing slogan devoid of clinical trial backing, it was subsequently retrofitted with a theoretical physiological rationale by Dr. Yoshiro Hatano, a researcher and professor at the Kyushu University of Health and Welfare. During the 1960s, Dr. Hatano and his research team became increasingly concerned about the shifting demographics of Japanese physical activity and the associated rise in metabolic syndrome. They began to investigate the typical ambulatory habits of the Japanese population across various lifestyles. The research team determined through observation that the average Japanese adult accrued between 3,000 to 5,000 steps per day as a baseline of incidental movement resulting from activities of daily living.
Operating on the principles of energy balance and caloric expenditure, Dr. Hatano hypothesized that increasing this baseline step count to the marketed 10,000 steps per day would result in an additional caloric expenditure of approximately 300 to 400 kilocalories (kcal) per day. The exact caloric burn would naturally fluctuate depending on an individual’s gait speed, stride length, body mass, gender, and age, but the mathematical average provided a solid heuristic. In standard metabolic terms, achieving 10,000 steps per day translated to an estimated energy expenditure of roughly 5 Metabolic Equivalent of Task hours (MET/h) for an average middle-aged Japanese man.
The research team postulated that maintaining this specific daily caloric deficit through increased locomotion would be highly sufficient to mitigate the creeping onset of obesity, improve systemic lipid profiles, and thereby significantly decrease the population-level risk of coronary artery disease. While Dr. Hatano’s energetic calculations were mathematically sound for that specific demographic and represented a logical preventative health hypothesis, there was absolutely no longitudinal mortality data at the time to confirm that 10,000 steps represented a biological threshold, an optimal plateau, or a universal necessity for health.
Nevertheless, the sheer simplicity of the metric allowed it to bypass rigorous scientific scrutiny. The concept of walking 10,000 steps provided a tangible, easily measurable target that did not require complex heart rate calculations, specialized athletic equipment, or gym memberships. Over the subsequent four decades, major international health bodies, including the World Health Organization, the American Heart Foundation, and the US Department of Health & Human Services, gradually integrated the 10,000-step target into their broad public health recommendations, effectively cementing a commercial trademark from 1965 as a global medical directive.
Methodological Evolution in Movement Epidemiology
To appreciate the recent paradigm shift regarding optimal step counts, one must first understand the profound methodological evolution in how physical activity is quantified in epidemiological research. For decades, the vast majority of physical activity data was derived from self-reported questionnaires. Participants in cohort studies would be asked to estimate the frequency, duration, and intensity of their walking and exercise habits over previous weeks or months. This methodology was inherently flawed, suffering heavily from recall bias, social desirability bias (where participants overestimate their activity levels to appear healthier), and a fundamental inability to accurately capture the incidental, non-exercise steps that occur during daily domestic or occupational tasks.
The advent of triaxial accelerometry and commercial wearable technologies in the early 21st century revolutionized the field of physical activity epidemiology. Unlike early mechanical pendulum pedometers—which were prone to significant error rates and could not distinguish between intentional walking and the incidental vibration of riding in a vehicle—modern digital accelerometers capture movement across three spatial planes. Devices such as the ActiGraph, deployed in massive studies like the National Health and Nutrition Examination Survey (NHANES) and the UK Biobank, continuously record the exact frequency, duration, and intensity of human locomotion.
This transition from subjective estimation to objective, device-measured data has allowed researchers to construct highly accurate, non-linear restricted cubic spline models. These sophisticated statistical models map step volume directly against verified mortality registries, utilizing Cox proportional hazards regression analyses to calculate precise hazard ratios (HRs) while adjusting for a multitude of confounding variables such as age, sex, race, education, diet, smoking status, body mass index, and pre-existing comorbidities. The resulting data provides a forensic view of how every single step impacts human biology over decades of follow-up.
Deconstructing the Dose-Response Curve for All-Cause Mortality
Leveraging device-based accelerometry, recent large-scale prospective cohort studies and subsequent international meta-analyses have systematically deconstructed the relationship between daily step volume and all-cause mortality. The absolute consensus across these massive datasets is definitive: there is a remarkably strong inverse association between daily step count and premature death. However, the risk reduction operates on a distinct curvilinear trajectory of diminishing marginal returns, rather than a linear trajectory up to 10,000 steps.
The Women’s Health Study (Lee et al., 2019)
Among the first major investigations to challenge the 10,000-step dogma using objective accelerometer data was a prospective cohort study published in JAMA Internal Medicine, led by Dr. I-Min Lee and researchers from Brigham and Women’s Hospital and Harvard Medical School. This study examined 16,741 older American women from the Women’s Health Study, with an average participant age of 72 years. The participants wore an accelerometer on their hip during waking hours for seven days, and mortality outcomes were tracked over a median follow-up of 4.3 years.
The findings of this study fundamentally dismantled the absolute necessity of the 10,000-step threshold for older populations. The researchers discovered that women who accrued merely 4,400 steps per day exhibited a staggering 41% lower risk of all-cause mortality compared to the least active baseline group, who averaged only 2,700 steps per day. The mortality risk continued to decrease in a dose-dependent manner as step volume increased beyond 4,400, but this risk reduction definitively plateaued at approximately 7,500 steps per day. Steps taken beyond the 7,500 threshold yielded no statistically significant additional mortality benefit in this specific older female cohort, indicating a biological ceiling for the survival benefits of step volume.
The Steps for Health Collaborative (Paluch et al., 2022)
To provide a more universally applicable assessment across diverse demographics, an exhaustive meta-analysis was published in The Lancet Public Health in 2022. The research team harmonized participant-level data from 15 separate international cohorts, encompassing a total sample of 47,471 adults (aged ≥ 18 years). Over a median follow-up of 7.1 years, representing 297,837 person-years of observation, the researchers recorded 3,013 deaths.
Using inverse-variance weighted random effects models, the investigators calculated adjusted hazard ratios across study-specific quartiles. The analysis provided irrefutable evidence of the profound efficacy of step volumes significantly lower than 10,000.
Table 1: Comparative Hazard Ratios of Step Volume on All-Cause Mortality (Paluch et al., 2022)
| Step Volume Quartile | Median Steps per Day | Adjusted Hazard Ratio (HR) | 95% Confidence Interval | Corresponding Mortality Risk Reduction |
|---|---|---|---|---|
| Quartile 1 (Reference) | 3,553 steps/day | 1.00 | N/A | Baseline Reference |
| Quartile 2 | 5,801 steps/day | 0.60 | 0.51 – 0.71 | 40% Reduction in Risk |
| Quartile 3 | 7,842 steps/day | 0.55 | 0.49 – 0.62 | 45% Reduction in Risk |
| Quartile 4 | 10,901 steps/day | 0.47 | 0.39 – 0.57 | 53% Reduction in Risk |
(Data derived from the meta-analysis of 15 international cohorts )
This data demonstrates that transitioning from the lowest quartile to just 5,801 steps per day eliminates nearly half of the premature mortality risk. The incremental benefit of adding another 5,000 steps to reach Quartile 4 only yields an additional 13% reduction, heavily illustrating the concept of diminishing marginal returns in physical activity epidemiology.
The Banach et al. Global Meta-Analysis (2023)
The epidemiological window was expanded further by a massive meta-analysis published in the European Journal of Preventive Cardiology, which evaluated 17 cohort studies involving a total of 226,889 participants with a median follow-up of 7.1 years. This study uniquely evaluated health benefits at the extreme upper end of the step distribution, analyzing data up to 20,000 steps per day.
The researchers established explicit minimum “cut-off” points where significant health benefits officially commence. For all-cause mortality, the minimum threshold was identified at merely 3,867 steps per day. Above this baseline, the researchers determined that every 1,000-step daily increment was associated with a 15% decreased risk of all-cause mortality (Hazard Ratio 0.85; 95% CI 0.81–0.91; P < 0.001).
A critical divergence in the Banach et al. findings compared to the Lee and Paluch studies is the observed absence of an upper plateau. While earlier meta-analyses capped their evaluations at approximately 13,000 to 15,000 steps—and subsequently observed statistical plateaus around the 8,000 to 10,000 mark—Banach’s team noted a continuous inverse association with a “more the better” trend even at the extreme upper tail of the distribution. However, the researchers concede a critical statistical limitation: the participant data for step counts exceeding 15,000 and approaching 20,000 per day remains statistically sparse. Consequently, the continuous linear benefit observed at this extreme high end requires further validation in larger cohorts before it can be considered conclusive.
The Curvilinear Reality of Locomotion
The underlying consensus across all these massive datasets is the presence of a non-linear, curvilinear dose-response relationship. The steepest and most profound phase of mortality risk reduction occurs at the absolute lower end of the distribution. Transitioning from a highly sedentary, inactive state (e.g., 2,000 steps) to a modestly active state (e.g., 4,000 to 5,000 steps) yields the most dramatic proportional improvement in lifespan.
This specific curve dynamics suggests that public health initiatives focused on transitioning the most sedentary individuals into light, achievable activity will yield far greater aggregate population health benefits than attempting to convince moderately active individuals to reach the arbitrary 10,000-step threshold. As noted by researchers in the field, taking more steps, particularly among those who are the least active, inherently provides the greatest absolute benefit to public health.
Age-Stratified Asymptotes: The Biology of Aging and Movement
A primary, highly consistent insight derived from the recent pooling of epidemiological data is that the optimal daily step volume is not monolithic; rather, it is heavily modified by chronological age. Restricted cubic spline models generated in recent meta-analyses reveal that the point at which mortality benefits plateau differs significantly between older and younger cohorts, reflecting deep underlying changes in human biology.
According to the Paluch et al. (2022) meta-analysis, the risk of all-cause mortality progressively decreases but then levels off at distinct, divergent points based on age stratification:
- Older Adults (Aged ≥ 60 years): The mortality benefit plateau occurs relatively early, between 6,000 and 8,000 steps per day.
- Younger Adults (Aged < 60 years): The mortality benefit continues to accumulate for a longer duration, plateauing higher at between 8,000 and 10,000 steps per day.
These exact findings are closely corroborated by the Banach et al. (2023) global analysis. The Banach data demonstrated that while the relative risks (RRs) of mortality were generally lower in older adults, the sharpest phase of risk reduction occurred at approximately 6,000 to 10,000 steps per day for those aged 60 and over (yielding a 42.3% risk reduction). In contrast, for participants under 60 years of age, the sharpest phase of risk reduction required a higher volume, occurring at approximately 7,000 to 13,000 steps per day (yielding a 48.7% risk reduction).
Table 2: Age-Stratified Optimal Step Thresholds for All-Cause Mortality
| Demographic Age Cohort | Minimal Effective Dose | Peak Risk Reduction Phase | Optimal Plateau Range |
|---|---|---|---|
| Younger Adults (< 60 years) | ~4,000 steps/day | 7,000 – 13,000 steps/day | 8,000 – 10,000+ steps/day |
| Older Adults (≥ 60 years) | ~3,800 steps/day | 6,000 – 10,000 steps/day | 6,000 – 8,000 steps/day |
(Compiled from stratified data models )
Physiological Correlates of the Age Discrepancy
The divergence in optimal stepping thresholds across age groups is not merely a statistical artifact of the datasets, but a direct reflection of the underlying biological realities related to the pathophysiology of aging.
Firstly, as individuals age, standard gait biomechanics and overall metabolic efficiency decrease significantly. This is primarily driven by sarcopenia (the age-related loss of skeletal muscle mass and strength), decreased joint mobility, reduced tendon elasticity, and alterations in neuromuscular recruitment patterns. Consequently, the absolute metabolic cost of walking a single step is measurably higher in a 75-year-old compared to a 35-year-old. Therefore, older adults achieve an equivalent cardiovascular and metabolic stimulus at a lower absolute volume of steps. The physiological stimulus required to upregulate endothelial nitric oxide synthase, improve cellular insulin sensitivity, and reduce systemic inflammation is reached earlier in the step count continuum.
Secondly, older populations inherently harbor a higher baseline burden of accumulated allostatic load, subclinical pathologies, and clinical morbidities, including osteoarthritis, peripheral artery disease, and chronic obstructive pulmonary disease. In these specific demographics, prescribing extreme volumes of ambulatory activity (e.g., pushing beyond 8,000 or 10,000 steps) may precipitate orthopedic degradation, joint inflammation, or cardiovascular overexertion that paradoxically counteracts the cardioprotective benefits of the movement.
Finally, the absolute baseline risk of mortality is naturally higher in older adults. Therefore, even small absolute increases in daily physical activity (e.g., transitioning from 3,000 to 6,000 steps) exert a massive, disproportionate prophylactic effect against the most imminent causes of mortality, such as acute myocardial infarction or ischemic stroke, maximizing the observable survival benefit at a lower threshold.
Cardiovascular and Oncological Risk Reduction Mechanisms
While all-cause mortality provides a crucial macro-level view of lifespan extension, analyzing the impact of step volume on specific pathogenic pathways—namely, cardiovascular disease (CVD) and oncological incidence—provides necessary insight into the systemic, cellular mechanisms of ambulatory activity.
Cardiovascular Disease (CVD) Prevention
The cardiovascular benefits of daily stepping manifest at remarkably low ambulatory volumes. The Banach et al. analysis established that the absolute minimum threshold required to begin observing statistically significant reductions in cardiovascular mortality is only 2,337 steps per day. Beyond this minimal threshold, every 500-step daily increment is associated with a highly significant 7% decrease in the risk of CV mortality (Hazard Ratio 0.93; 95% CI 0.91–0.95; P < 0.001).
Compared with the lowest reference quartile for cardiovascular outcomes (median 2,337 steps/day), higher step volumes resulted in massive, dose-dependent reductions in CV mortality risk:
- Quartile 1 (median 3,982 steps/day): 16% reduced risk of CV mortality.
- Quartile 2 (median 6,661 steps/day): 49% reduced risk of CV mortality.
- Quartile 3 (median 10,413 steps/day): 77% reduced risk of CV mortality.
These findings underscore the exquisite sensitivity of the human cardiovascular system to mechanotransduction. Even low-volume ambulation induces vital sheer stress on the vascular endothelium. This sustained mechanical stress promotes the release of vasodilators like nitric oxide, actively reduces arterial stiffness, lowers ambulatory blood pressure, and mitigates the progression of atherosclerosis.
Further robust evidence of low-volume efficacy in high-risk populations is found in the NAVIGATOR trial (Nateglinide and Valsartan in Impaired Glucose Tolerance Outcomes Research), meticulously analyzed by Yates et al. in The BMJ. This prospective cohort focused on 9,306 individuals spanning 40 countries who presented with impaired glucose tolerance alongside existing cardiovascular disease or high CVD risk factors. Utilizing research-grade pedometers, the researchers found that in this highly vulnerable population, each 2,000-step increment in average daily activity—up to a cap of 10,000 steps—was associated with a 6% relative risk reduction in the progression to full type 2 diabetes mellitus.
This powerful data confirms that even minor, incremental behavioral adjustments (such as adding a standard 20-minute walk to one’s daily routine) can fundamentally alter the glycemic trajectory of pre-diabetic patients. Ambulatory movement relies heavily on the contraction of large skeletal muscles in the lower extremities, which triggers the insulin-independent translocation of GLUT4 transporters to the cell membrane, rapidly clearing glucose from the bloodstream and reducing the metabolic burden on the pancreas.
Oncological Incidence and Mortality
The interplay between physical activity volume and cancer biology is highly complex, mediated primarily through the regulation of systemic adiposity, the modulation of endogenous sex hormones (such as circulating estrogen and androgens), and the suppression of systemic chronic inflammation and oxidative stress. A massive, population-based prospective cohort study authored by Del Pozo Cruz et al. (2022) and published in JAMA Internal Medicine utilized comprehensive data from 78,500 individuals in the UK Biobank to assess step volume against the specific incidence of 13 cancers known to be intrinsically associated with physical inactivity.
The restricted cubic spline regression models utilized in the analysis revealed that up to approximately 10,000 steps per day, there were consistent, measurable declines in both the overall incidence and the subsequent mortality rates of the composite cancer outcomes. Interestingly, the optimal risk reduction threshold for the cancer composite clustered much closer to the 10,000-step mark than the cardiovascular markers did, suggesting that effective oncological prophylaxis may inherently require a higher total daily energy expenditure to fully optimize metabolic homeostasis, regulate endocrine function, and maintain robust immune surveillance mechanisms.
Neuroprotection and the Preservation of Cognitive Reserve
Perhaps the most compelling and rapidly evolving recent discoveries regarding ambulatory step volume relate to neurodegeneration and cognitive preservation. Until recently, explicit, device-measured data quantifying the precise dose-response relationship between objective daily step counts and incident dementia was severely lacking in the neurological literature.
In 2022, Del Pozo Cruz and colleagues filled this epidemiological void by publishing a landmark study in JAMA Neurology. This study again utilized the massive UK Biobank dataset, isolating 78,430 adults aged 40 to 79 who were entirely free of cognitive impairment at the baseline, and tracking their outcomes over a 7-year median follow-up period. The complex analysis mapped continuous accelerometer data against the clinical onset of all-cause dementia, revealing profound protective effects linked directly to step volume.
Table 3: Dose-Response Relationship for Incident Dementia
| Step Volume Parameter | Daily Step Count | Corresponding Hazard Ratio (HR) | Reduction in Incident Dementia Risk |
|---|---|---|---|
| Minimal Effective Dose | 3,826 steps/day | 0.75 (95% CI, 0.67-0.83) | 25% Reduction |
| Optimal Protective Dose | 9,826 steps/day | 0.49 (95% CI, 0.39-0.62) | 51% Reduction |
(Data derived from the JAMA Neurology UK Biobank analysis )
As demonstrated, accumulating merely 3,826 steps per day was associated with a highly significant 25% reduction in the risk of developing incident dementia. The maximum observable risk reduction—effectively halving the risk of dementia incidence—was observed at an optimal dose of 9,826 steps per day. Beyond this specific numerical point, the neuroprotective benefits statistically leveled off, providing no further cognitive advantage.
These epidemiological findings are profoundly coherent with established neurobiology. A highly significant proportion of all-cause dementia is driven by microvascular pathologies (often categorized as vascular dementia) and the gradual degradation of the blood-brain barrier. Ambulatory activity directly enhances cerebral blood perfusion, ensuring adequate oxygenation of neural tissues. Furthermore, sustained aerobic movement upregulates the expression of Brain-Derived Neurotrophic Factor (BDNF), a vital protein that facilitates synaptogenesis and neurogenesis, particularly within the hippocampus, the brain’s primary memory center. Lastly, the improvement in systemic glycemic control provided by walking is critical, given the increasing characterization of Alzheimer’s disease as “Type 3 diabetes,” wherein cerebral insulin resistance precipitates amyloid plaque accumulation. The finding that roughly 9,800 steps represents the neuroprotective zenith suggests that while 10,000 steps originated as a marketing myth, it serendipitously aligns almost perfectly with the biological maximum for cognitive preservation in aging adult populations.
The Sedentary Time Interaction: Can Stepping Counteract Sitting?
A critical, independent variable that frequently confounds step-count data is the baseline amount of time an individual spends in an entirely sedentary state. In modern occupational environments, it is increasingly common for an individual to achieve an optimal 8,000 to 10,000 steps—perhaps through a dedicated 60-minute morning run or gym session—but spend the remaining 11 hours of their waking day seated motionlessly at a desk or in a vehicle. This specific behavioral pattern—often termed the “active couch potato” phenomenon in kinesiology—raises a vital epidemiological question: can high step volumes fully offset the independent, deleterious physiological effects of prolonged, uninterrupted sedentary time?.
A comprehensive 2024 analysis by Ahmadi et al., published in the British Journal of Sports Medicine, addressed this exact interaction utilizing device-based cohort data with an average follow-up of 6.9 years. The researchers statistically stratified participants into two distinct categories based on an identified inflection point of absolute risk: a “high sedentary time” group (those sedentary for ≥ 10.5 hours/day) and a “low sedentary time” group (those sedentary for < 10.5 hours/day).
The dose-response analysis revealed that while high sedentary time inherently elevates the baseline risk of mortality and cardiovascular events, accumulating a sufficient stepping volume can indeed counteract the pathology of prolonged sitting. For individuals relegated to the high sedentary category, the researchers observed the following parameters:
- The minimal threshold required to substantially lower mortality and CVD risk was determined to be between 4,000 and 4,500 steps/day (with an HR of 0.90 for all-cause mortality at 4,300 steps).
- The optimal protective dose (the absolute nadir of the risk curve) was observed between 9,000 and 10,000 steps/day. Specifically, the optimal dose for CVD risk reduction in highly sedentary individuals was 9,700 steps/day.
- Accruing this optimal 9,000 to 10,000 steps/day in highly sedentary individuals effectively lowered the absolute risk of all-cause mortality by 39% and incident CVD by 21% when compared to the lowest stepping baseline of 2,200 steps/day.
Interestingly, the researchers found that there was absolutely no effect modification by sedentary time levels on the fundamental shape of the dose-response curve for daily steps; the trajectory of “more steps equals lower risk” remained universally consistent regardless of sitting time. However, the absolute risk for a given step count was always slightly higher in the high-sedentary group compared to the low-sedentary group. The profound public health conclusion derived from this data is that accruing approximately 10,000 steps serves as a highly effective, necessary biological countermeasure to the unique pathology of extended, occupational sitting.
The Cadence Controversy: Volume Versus Stepping Intensity
As accelerometry swiftly replaced mechanical pedometry over the last decade, epidemiological researchers gained the unprecedented ability to measure not just how many steps an individual takes throughout a 24-hour period, but exactly how fast they take them. This technological leap led to a fierce and highly nuanced debate within the fields of kinesiology and epidemiology: does the absolute intensity of walking (measured as cadence) provide independent, additive health benefits beyond the mere total volume of steps?.
Defining Standardized Intensity Metrics
To effectively study intensity, step cadence (steps per minute) is typically quantified into established heuristic thresholds, allowing researchers to categorize physical exertion without relying on heart rate monitors or maximal oxygen uptake (VO2 max) testing. The primary metrics include:
- Incidental Steps: < 40 steps/min (representing light movement, such as slow walking around the house or office).
- Purposeful Steps: ≥ 40 steps/min (representing intentional, continuous locomotion).
- Moderate Intensity Walking: Generally defined as ≥ 100 steps/min, though heuristic thresholds can range between 90 to 125 steps/min depending on the specific age group being analyzed.
- Vigorous Intensity Walking: Generally defined as ≥ 130 steps/min.
- Peak-30 Cadence: A crucial epidemiological metric defined as the average steps/min recorded during the 30 highest, but not necessarily consecutive, minutes of stepping throughout a single day.
The Null Intensity Hypothesis (Volume is King)
A highly robust subset of the most comprehensive meta-analyses currently available concludes that once the total daily step volume is statistically accounted for, step intensity entirely loses its statistical significance regarding the primary endpoint of all-cause mortality.
In the Saint-Maurice et al. (2020) analysis utilizing a representative sample of US adults from the NHANES database, researchers found that greater step intensity was simply not significantly associated with lower mortality after applying rigorous statistical adjustments for the total number of steps per day. When comparing the highest versus the lowest quartile of peak-30 cadence, the adjusted hazard ratio was 0.90 (95% CI, 0.65-1.27), and the P value for the trend was 0.34, rendering the benefit statistically non-significant.
Similarly, the Women’s Health Study analysis by Lee et al. (2019) found that while higher stepping intensities initially appeared to lower mortality rates in older women in raw, unadjusted models, the associations were entirely attenuated and rendered non-significant after the statistical models were adjusted for total steps per day. The exhaustive Paluch et al. (2022) Lancet meta-analysis echoed this exact phenomenon, noting that when adjusting for volume, stepping rate was no longer significantly associated with time spent walking at moderate or higher paces.
The overarching biological implication of the Null Intensity Hypothesis is that for the ultimate, macro-level endpoint of lifespan extension, how much an individual moves is vastly more important than how fast they move. According to these models, a slow, incidental accumulation of 8,000 steps throughout an active workday confers virtually the exact same long-term mortality benefit as a rapid, purposeful 8,000-step power walk.
The Pro-Intensity Hypothesis (Cadence Enhances Healthspan)
Conversely, another prominent faction of the epidemiological literature—spearheaded by the massive UK Biobank cohort studies authored by Del Pozo Cruz—argues that stepping intensity provides independent, additive benefits that cannot be ignored, particularly for highly specific, quality-of-life morbidities.
In their 2022 UK Biobank analyses, Del Pozo Cruz et al. demonstrated that peak-30 cadence was consistently associated with notably lower risks of cancer incidence, cardiovascular disease incidence, and incident dementia, functioning completely beyond the benefit provided by the total daily steps. For dementia in particular, the data was stark: steps performed at a deliberately higher intensity resulted in much stronger inverse associations with cognitive decline, suggesting that neuroprotection specifically requires periods of elevated heart rate and maximum cerebral perfusion.
Furthermore, research explicitly investigating intermediate cardiometabolic markers strongly supports the vital, independent role of cadence. A detailed study examining step count volume versus intensity found that a significantly greater number of immediate cardiometabolic risk factors were positively associated with step intensity rather than step volume. Higher peak 30-minute and 60-minute cadences (spanning the moderate and high tertiles) were significantly and consistently associated with a lower body mass index (BMI), notably reduced waist circumference, lower systolic and diastolic blood pressures, and higher circulating levels of high-density lipoprotein (HDL) cholesterol. In stark contrast, isolated step volume without intensity was largely only significantly associated with lower circulating triglyceride levels.
Synthesizing the Contradiction: Lifespan vs. Healthspan
The apparent contradiction in the literature regarding cadence can be logically reconciled by carefully distinguishing between the specific clinical endpoints being measured. Total step volume is definitively the primary driver of reducing all-cause mortality, thereby dictating overall lifespan. However, stepping intensity appears to be the primary, indispensable driver for modulating intermediate physiological markers (such as body composition, lipid profiles, and vascular compliance) and directly reducing the incidence of highly specific, complex pathologies like vascular dementia and Alzheimer’s, thereby dictating overall healthspan. Therefore, while a slow, high-volume walk may keep a patient alive just as long as a fast, high-volume walk, the faster walk will almost certainly result in a significantly leaner body mass, superior cholesterol ratios, greater cardiovascular reserves, and a more robust cognitive capacity in their final decades.
Public Health Implications and Clinical Translation
The rigorous epidemiological deconstruction of the 10,000-step myth necessitates a profound paradigm shift in how global public health guidelines, specific clinical prescriptions, and consumer wearable manufacturers approach and communicate ambulatory behavior.
The rigid adherence to an arbitrary 10,000-step threshold can paradoxically act as a severe psychological barrier to physical activity initiation. For highly sedentary populations, the frail elderly, or individuals managing complex chronic illnesses, an absolute daily goal of 10,000 steps may appear entirely insurmountable. This perception often leads to a phenomenon of total non-compliance, where individuals opt for total inactivity because the perceived optimal target is out of reach. The cumulative data clearly and repeatedly demonstrates that the steepest and most clinically vital phase of mortality risk reduction occurs at the absolute lowest end of the movement spectrum.
Consequently, clinical messaging and public health policy must transition away from absolute, universal targets and pivot toward relative, incremental micro-prescriptions. Moving an inactive individual from a baseline of 2,000 steps to just 4,000 steps yields a far greater proportional benefit to aggregate public health than moving a moderately active individual from 8,000 to 10,000 steps. As explicitly noted in the clinical interpretation of the massive Banach and Paluch datasets, primary care clinicians should focus exclusively on prescribing manageable 1,000-to-2,000 step increments slightly above the patient’s current, individualized baseline. By establishing incremental goals (e.g., advising a patient currently walking 4,000 steps to aim for 5,000, and then eventually 6,000), practitioners can capitalize on the highly significant 15% reduction in all-cause mortality that is statistically associated with that simple 1,000-step addition. These minor, relative improvements are exponentially more achievable, sustainable, and psychologically palatable for patients than a daunting 10,000-step mandate.
Conclusions
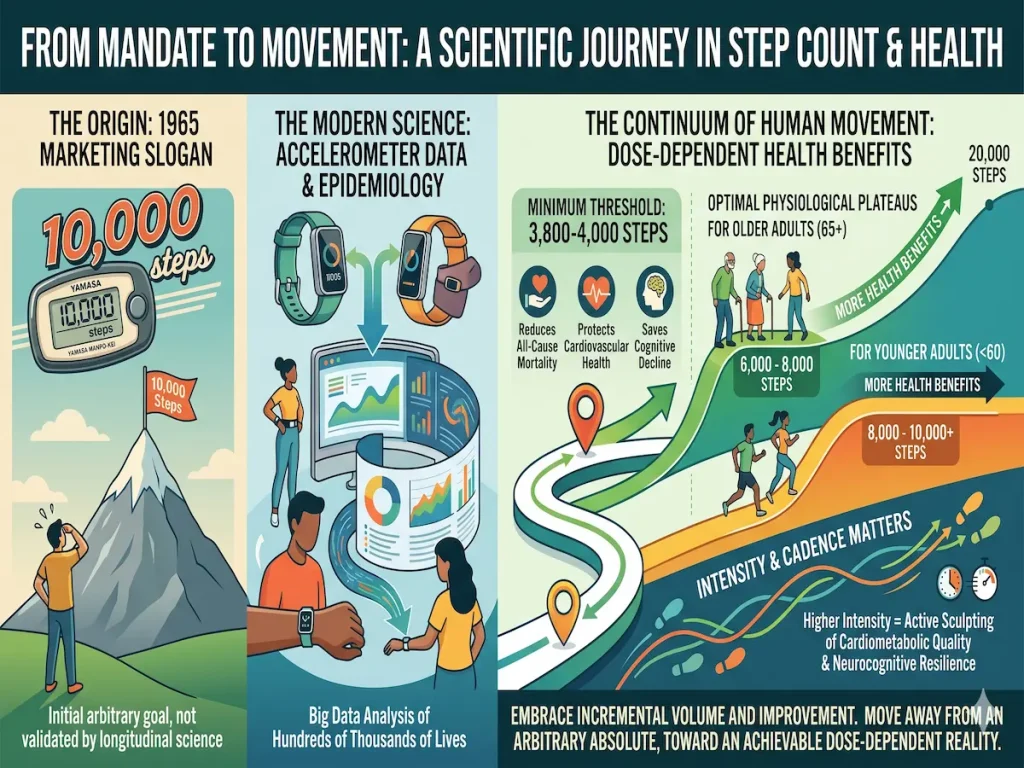
The “10,000 steps a day” mandate serves as a fascinating, highly impactful case study in the intersection of corporate marketing, technological evolution, and global public health epidemiology. Originating as a clever visual pun and marketing slogan for the 1965 Japanese Yamasa Manpo-kei pedometer, the metric successfully galvanized a sedentary global population long before longitudinal, device-measured science possessed the capability to validate it.
However, contemporary epidemiological analysis utilizing sophisticated wrist and hip-worn accelerometers across hundreds of thousands of lives reveals a much more accessible, highly nuanced biological reality. While the inverse association between stepping and mortality remains mathematically robust up to an impressive 20,000 steps, the essential physiological threshold for profound lifespan preservation sits remarkably low. An accumulation of merely 3,800 to 4,000 steps establishes a highly powerful prophylactic shield against all-cause mortality, cardiovascular degradation, and cognitive decline.
The optimal physiological plateau for these benefits is intricately bound to biological age and physical capacity, capping early at 6,000 to 8,000 steps for older adults, and stretching higher to 8,000 to 10,000+ steps for younger adults. Furthermore, while the absolute volume of daily locomotion dictates the raw extension of longevity, the intensity and cadence of that locomotion actively sculpts the cardiometabolic quality and neurocognitive resilience of those living years. The 10,000-step goal is definitively not a myth in terms of its absolute biological utility—particularly for counteracting the unique, modern crisis of prolonged occupational sedentary time, or for strictly optimizing neuroprotection against dementia—but it is unequivocally a myth that it represents the scientific baseline required for human health. By fully embracing the epidemiological science of incremental volume and relative improvement, preventative medicine can successfully redefine human movement away from a daunting, arbitrary numerical absolute, and guide populations toward an achievable, highly effective, dose-dependent continuum.
Reference: Lee, I-M., et al. (2019). Association of Step Volume and Intensity With All-Cause Mortality. JAMA Internal Medicine.