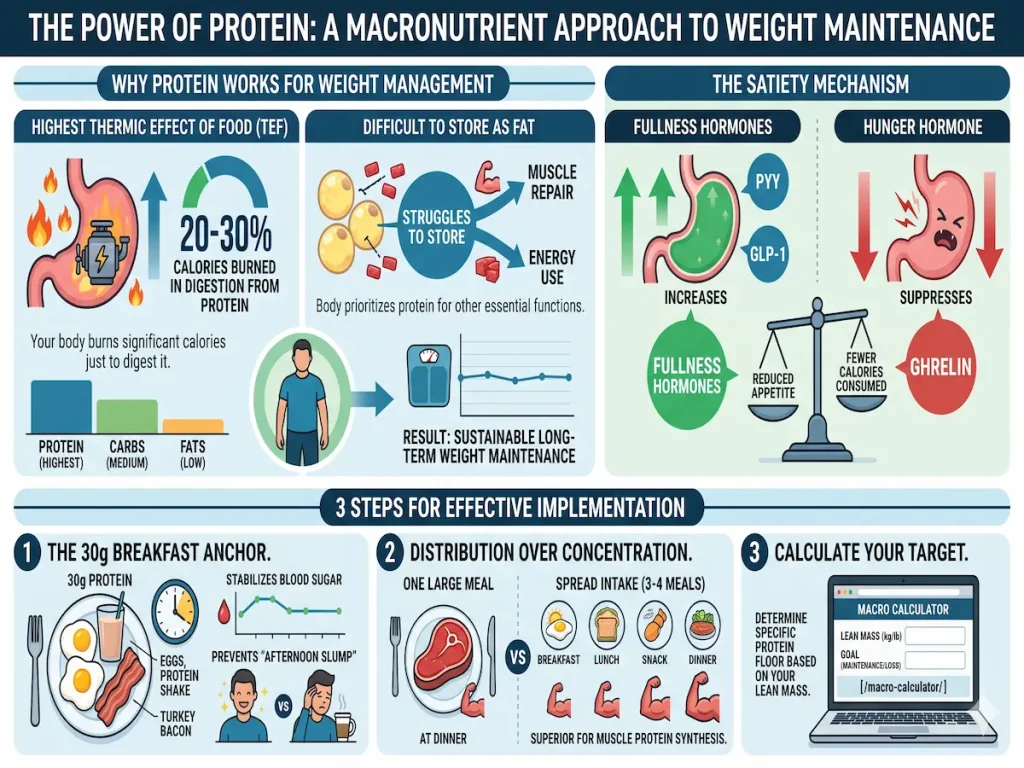
Protein is the only macronutrient that the body struggles to store as fat. It also has the highest **Thermic Effect of Food (TEF)**—meaning your body burns about 20–30% of the calories in protein just to digest it.
The Satiety Mechanism
Protein triggers the release of PYY and GLP-1 (fullness hormones) while suppressing Ghrelin (the hunger hormone). This makes high-protein diets the most sustainable “hack” for long-term weight maintenance.
The Implementation
1.The 30g Breakfast Anchor: Starting the day with 30g of protein stabilizes blood sugar and prevents the “afternoon slump.”
2. Distribution over Concentration: Research suggests that spreading protein intake across 3–4 meals is superior for muscle protein synthesis than one large meal.
3.Calculate Your Target:Use our [Macro Calculator](/macro-calculator/) to determine your specific protein floor based on your lean mass.
A Comprehensive Analysis of Macronutrient Utilization
The physiological assimilation, utilization, and storage of dietary macronutrients are governed by distinct, highly regulated biochemical pathways. Among the three primary macronutrients, dietary protein exhibits anomalous thermodynamic and structural properties. Unlike carbohydrates and lipids, which serve predominantly as primary oxidative fuels and energy storage molecules, protein functions fundamentally as a structural and functional substrate. The human body demonstrates a profound biological resistance to sequestering dietary protein into adipose tissue. This resistance is mediated through a complex, multi-tiered interplay of elevated thermogenesis, metabolically inefficient biochemical conversion pathways, and potent neuroendocrine feedback loops that collectively suppress appetite, upregulate energy expenditure, and partition energy toward tissue remodeling.
An exhaustive evaluation of current nutritional biochemistry, clinical endocrinology, and sports dietetics reveals that optimizing protein intake—both in absolute quantity and in chronological distribution—is a fundamental strategy for optimizing body composition, maintaining glycemic control, and promoting long-term metabolic health. The subsequent analysis comprehensively deconstructs the thermodynamic cost of protein metabolism, the neurobiological mechanisms of protein-induced satiety, the clinical efficacy of morning protein anchoring, the current paradigms regarding muscle protein synthesis and meal distribution, and the precise calculation of individualized protein requirements based on fat-free mass.
The Thermodynamics of Macronutrient Metabolism and the Thermic Effect of Food
Energy expenditure in the human body is compartmentalized into three primary domains: basal metabolic rate (BMR), activity-induced energy expenditure (AIEE), and diet-induced thermogenesis (DIT), which is synonymous with the Thermic Effect of Food (TEF). The TEF represents the obligatory caloric expenditure required for the mechanical and enzymatic digestion, intestinal absorption, systemic assimilation, and ultimate storage or oxidation of nutrients following a postprandial ingestion event.1 When evaluating the thermodynamic efficiency of the human diet, it becomes immediately apparent that the macronutrient composition of an ingested meal profoundly alters the magnitude of the thermogenic response.
Comparative Thermogenesis and Metabolic Inefficiency
Dietary fat is highly efficient for the body to digest, transport, and store. The transfer of ingested dietary triglycerides into adipocyte storage requires minimal biochemical alteration, resulting in an exceptionally low TEF ranging from 0% to 3% of the total ingested lipid calories.1 Carbohydrate metabolism demands a moderate degree of energy, primarily due to the active transport mechanisms required to move glucose across the intestinal lumen and the enzymatic cost associated with hepatic and skeletal glycogen synthesis. This yields a TEF of approximately 5% to 10%.1
Conversely, the processing of dietary protein is remarkably energy-intensive, possessing a TEF of 20% to 30%.1 This uniquely high thermogenic response indicates that up to nearly one-third of the caloric energy derived from ingested protein is immediately dissipated as heat during its metabolic processing. To contextualize this, if an individual consumes 100 kilocalories of pure protein, the net metabolizable energy available to the body is only 70 to 80 kilocalories, as the remainder is expended simply to process the nutrient itself.2
| Macronutrient | Energy Density (kcal/g) | Thermic Effect of Food (TEF %) | Primary Postprandial Fate |
| Dietary Fat | 9 | 0 – 3% | Peripheral and hepatic triglyceride storage, oxidative fuel |
| Carbohydrate | 4 | 5 – 10% | Hepatic and skeletal glycogen synthesis, oxidative fuel, lipogenesis |
| Protein | 4 | 20 – 30% | Muscle protein synthesis, cellular tissue turnover, gluconeogenesis |
Biochemical Drivers of Protein Thermogenesis
The elevated adenosine triphosphate (ATP) consumption associated with protein ingestion is driven by several concurrent biochemical cascades that occur in the immediate postprandial period.2 Initially, the hydrolysis of complex, folded polypeptide chains into constituent dipeptides, tripeptides, and free amino acids within the acidic environment of the stomach and the enzymatic milieu of the small intestine requires extensive energy.2 Subsequently, the active transport of these amino acids across the intestinal epithelium against steep concentration gradients relies heavily on ATP-dependent cotransporters.
Furthermore, postprandial amino acid handling heavily involves the hepatic system. Because the human body lacks a dedicated, high-capacity storage reservoir for free amino acids (unlike glycogen for carbohydrates or adipocytes for lipids), excess amino acids must be rapidly metabolized to maintain physiological homeostasis. This metabolic disposal includes protein synthesis, an inherently ATP-expensive process requiring the charging of transfer RNA (tRNA) molecules and ribosomal translocation along messenger RNA (mRNA).3
Additionally, the clearance of nitrogenous waste via the urea cycle, termed ureagenesis, is highly energy-dependent, consuming four molecules of ATP for every molecule of urea synthesized.4 When dietary amino acids are diverted for energy production, they undergo deamination, and their carbon skeletons are utilized in gluconeogenesis (the de novo synthesis of glucose from non-carbohydrate precursors). Gluconeogenesis is thermodynamically demanding, requiring six equivalents of ATP to generate a single molecule of glucose from pyruvate or specific glucogenic amino acids.6 The cumulative ATP demand of protein synthesis, ureagenesis, and gluconeogenesis accounts for the profound postprandial thermogenesis observed following a high-protein meal, effectively reducing the net energy available for adipose storage.2
Further research into human thermogenesis indicates that physiological variables such as total body composition can influence the TEF. Clinical studies comparing lean and obese subjects have demonstrated that obese individuals often exhibit a blunted thermogenic response to dietary fat, sometimes as low as -0.9% to a negligible positive increase, compared to a robust 14.4% in lean subjects when evaluated under specific mixed-meal conditions.7 However, regardless of the individual’s metabolic baseline or body mass index (BMI), protein consistently yields the highest thermogenic output, solidifying its role as a metabolic catalyst that elevates resting energy expenditure (REE) during weight loss and weight maintenance phases.8
De Novo Lipogenesis: The Inefficiency of Protein-to-Fat Conversion
The widespread nutritional consensus that protein is the only macronutrient that the body struggles to store as fat is fundamentally grounded in the stoichiometry of De Novo Lipogenesis (DNL). DNL is a complex, highly regulated metabolic pathway that converts non-lipid carbon precursors into fatty acids, which are subsequently esterified with a glycerol backbone to form triacylglycerols (TAGs) for long-term storage in adipose tissue.10
The Stoichiometric Burden of De Novo Lipogenesis
While hepatic DNL is highly responsive to dietary carbohydrate surplus—particularly excess fructose and glucose, which readily supply acetyl-CoA and glycerol-3-phosphate under the transcriptional control of sterol regulatory element-binding protein-1c (SREBP-1c) and carbohydrate response element binding protein (ChREBP)—the conversion of dietary amino acids into fatty acids is exceedingly complex and energetically unfavorable.10
To synthesize a single molecule of palmitate, a 16-carbon saturated fatty acid that serves as the primary end-product of mammalian DNL, the biochemical cost is staggering. The process requires continuous cycling of the multi-enzyme fatty acid synthase (FAS) complex and acetyl-CoA carboxylase (ACC). The overall stoichiometric equation for the synthesis of palmitate dictates massive energy and cofactor inputs:

This biochemical reality demonstrates that seven molecules of ATP and fourteen molecules of NADPH (generated primarily via the pentose phosphate pathway) are consumed merely to construct the carbon backbone of one relatively short fatty acid.12 When dietary protein serves as the origin substrate for this pathway, the metabolic penalty is even steeper. The amino acids must first undergo transamination or oxidative deamination, which imposes an additional energy cost via the urea cycle to safely excrete the neurotoxic ammonia byproduct.18 Following deamination, the remaining carbon skeletons must be converted into intermediates of the tricarboxylic acid (TCA) cycle or into pyruvate, and eventually shuttled out of the mitochondria as citrate to be cleaved into cytosolic acetyl-CoA.19
Studies utilizing highly sensitive isotopic tracing methodologies in both in vitro human hepatocyte models and in vivo human subjects have revealed that while certain amino acids (such as glutamine, glutamate, and leucine) can contribute carbon to hepatic DNL, the absolute flux and conversion efficiency are minimal compared to carbohydrate-driven DNL.21 The metabolic cost of converting surplus protein into adipose tissue is estimated to dissipate over 25% to 30% of the substrate’s inherent energy, making it an evolutionarily disfavored pathway.12 Consequently, the human body prioritizes the oxidation of excess amino acids or their conversion to glucose, strictly limiting their integration into lipid droplets.
Clinical Evidence: Hypercaloric Protein Overfeeding Trials
The profound physiological resistance to fat accumulation from dietary protein has been robustly demonstrated in controlled clinical overfeeding trials. Under normal physiological conditions, continuous caloric surpluses lead unequivocally to fat mass accretion. Classical overfeeding literature establishes that fat overfeeding results in the storage of 90% to 95% of the excess calories as adipose tissue, while carbohydrate overfeeding results in 75% to 85% storage.25
However, overfeeding trials utilizing pure protein challenge this established thermodynamic paradigm. In a landmark randomized controlled trial conducted by Antonio et al., resistance-trained adult subjects were prescribed a hypercaloric diet featuring an astronomical protein intake of 4.4 grams per kilogram of body weight per day (approximately 5.5 times the standard Recommended Dietary Allowance).26 The high-protein cohort consumed an average daily surplus of over 800 kilocalories compared to their baseline maintenance intake for a continuous period of eight weeks, equating to an average intake of 307 grams of protein per day.26
Despite this massive, sustained caloric surplus, high-resolution body composition analysis via air displacement plethysmography (Bod Pod) revealed a startling outcome: there were no significant increases in body weight, fat mass, or body fat percentage compared to the control group, who maintained their habitual dietary intake.26 In fact, the high-protein group exhibited a slight, albeit non-significant, average loss of fat mass (-1.6 kg) despite the extreme caloric surplus.29
This distinct absence of fat mass gain in the presence of a severe protein-derived caloric surplus suggests profound metabolic adaptations unique to protein metabolism.30 Potential mechanisms explaining this massive energy dissipation include a significant upregulation of spontaneous physical activity or Non-Exercise Activity Thermogenesis (NEAT), adaptive thermogenesis driven by accelerated whole-body protein turnover, and the intrinsic thermodynamic inefficiency of amino acid-driven DNL.4 The empirical consensus drawn from these extreme feeding trials dictates that consuming excess calories in the form of protein yields fundamentally different morphometric and metabolic outcomes than equivalent caloric surpluses derived from carbohydrates or fats.33
The Neuroendocrine Satiety Mechanism: Gut-Brain Axis Integration
Beyond its metabolic inefficiency regarding lipogenesis, dietary protein constitutes the most highly satiating macronutrient due to its potent, multifaceted interaction with the enteroendocrine system.2 High-protein diets represent one of the most sustainable and effective biological “hacks” for long-term weight maintenance precisely because they fundamentally alter the neuroendocrine regulation of appetite, seamlessly replacing the psychological burden of voluntary caloric restriction with physiological satiation.8
Enteroendocrine Receptors and Apical Nutrient Sensing
The gastrointestinal tract is not merely an absorptive conduit; it is the largest endocrine organ in the human body. It is lined with specialized enteroendocrine cells (EECs), notably the L-cells, which are located predominantly in the distal ileum and colon, acting as the primary nutrient sensors of the digestive system.35 Upon the ingestion and subsequent gastric breakdown of protein, the resulting luminal concentration of peptones, oligopeptides, and free amino acids is detected by specific G-protein coupled receptors (GPCRs) situated on the apical membrane of these L-cells.36
The physiological detection of protein is orchestrated by several key receptors and transporters that mediate protein-induced satiety:
- Peptide Transporter 1 (PepT1): This is an electrogenic transporter that co-transports dietary dipeptides and tripeptides alongside protons into the enterocyte. This intracellular influx of positive charge induces membrane depolarization, which subsequently activates voltage-gated calcium channels, leading to a massive intracellular calcium influx that triggers hormone vesicle exocytosis.36
- Calcium-Sensing Receptor (CaSR): Activated predominantly by specific aromatic and branched-chain L-amino acids, the CaSR stimulates intracellular cyclic AMP (cAMP) production and phospholipase C pathways, further elevating intracellular calcium levels.37
- GPRC6A: A broadly tuned amino acid receptor that recognizes basic L-amino acids. Upon activation, it amplifies the intracellular cAMP signaling cascade, promoting cAMP response element-binding protein (CREB) phosphorylation, which regulates both the immediate secretion and the long-term genetic transcription of satiety hormones.38
| Receptor / Transporter | Primary Luminal Ligand | Intracellular Mechanism | Resulting Hormonal Output |
| PepT1 | Dipeptides, Tripeptides | Membrane depolarization, ERK1/2 pathway activation | GLP-1, PYY secretion |
| CaSR | L-amino acids | cAMP activation, Intracellular calcium efflux | GLP-1, CCK, PYY secretion |
| GPRC6A | Basic L-amino acids | CREB signaling, Intracellular calcium efflux | GLP-1, PYY secretion |
The Anorexigenic Cascade: GLP-1, PYY, and Ghrelin
The concerted activation of PepT1, CaSR, and GPRC6A triggers the rapid exocytosis of potent anorexigenic (appetite-suppressing) hormones into the systemic circulation, most notably Glucagon-Like Peptide-1 (GLP-1) and Peptide YY (PYY).42
- Glucagon-Like Peptide-1 (GLP-1): Secreted primarily by the L-cells, GLP-1 exerts peripheral effects by delaying gastric emptying (the “ileal brake” mechanism) and enhancing glucose-dependent insulin secretion from pancreatic beta cells. Crucially, GLP-1 also crosses the blood-brain barrier and binds to receptors within the hypothalamus and the brainstem (nucleus tractus solitarius), thereby severely suppressing the neurological drive to eat.35
- Peptide YY (PYY): Co-secreted alongside GLP-1, PYY functions as a critical neuroendocrine modulator. It actively inhibits orexigenic neuropeptide Y (NPY) and agouti-related peptide (AgRP) neurons while simultaneously activating anorexigenic pro-opiomelanocortin (POMC) pathways in the arcuate nucleus of the hypothalamus, enforcing a profound and prolonged state of satiety.9 Clinical observations confirm that PYY null mice are entirely resistant to the satiating effects of protein, underscoring its absolute necessity in the gut-brain axis.40
Simultaneously, high-protein intake exerts a powerful inhibitory effect on the secretion of Ghrelin, a 28-amino acid orexigenic hormone produced predominantly by the oxyntic cells of the gastric fundus.42 Ghrelin typically rises in the preprandial state, crossing the blood-brain barrier to stimulate growth hormone secretagogue receptors in the arcuate nucleus, inducing intense sensations of hunger.8 The suppression of ghrelin via dietary protein effectively eliminates the biological drive for subsequent food-seeking behavior.9
Therefore, the dual action of elevating anorexigenic hormones (GLP-1/PYY) while simultaneously suppressing the primary orexigenic hormone (Ghrelin) creates a synergistic endocrine environment highly conducive to establishing a sustainable, long-term caloric deficit without the exhaustive psychological friction associated with traditional dieting.8
The 30-Gram Breakfast Anchor: Glycemic Control and Corticolimbic Regulation
While absolute daily protein intake dictates overarching metabolic adaptations, the circadian timing of protein consumption significantly influences its immediate behavioral and endocrine outcomes. Epidemiological data indicates a high prevalence of breakfast skipping or the consumption of carbohydrate-dense, protein-poor morning meals in Western populations.45 Such dietary habits precipitate wide glycemic excursions, reactive hypoglycemia, and ensuing mid-day fatigue—commonly colloquially known as the “afternoon slump”.47 Anchoring the morning meal with an optimal protein threshold, specifically targeting approximately 30 grams, fundamentally rewires daily appetite regulation, metabolic stability, and cognitive stamina.
Mitigating Glycemic Variability and the Second-Meal Phenomenon
A breakfast anchored with 30 grams of high-quality protein effectively curtails rapid postprandial glucose spikes.49 High-protein meals delay gastric emptying and induce an early, robust release of incretin hormones, which orchestrate a more modulated, sustained insulin response.52 This prevents the precipitous drop in blood sugar that typically triggers mid-morning lethargy, brain fog, and severe cravings for simple carbohydrates.48
Furthermore, morning protein consumption exhibits a potent “second-meal phenomenon,” whereby the glycemic and incretin response to a subsequent lunch is vastly improved, establishing a stable metabolic milieu for the entire diurnal cycle.54 The stabilization of blood glucose mitigates the physiological stress response, buffering erratic cortisol spikes and preserving the natural cortisol awakening response.48 This hormonal baseline is vital for maintaining sustained cognitive focus and alertness.48 The amino acids provided in the morning, particularly tryptophan and tyrosine, also serve as direct metabolic precursors for the synthesis of critical neurotransmitters, including serotonin, dopamine, and gamma-aminobutyric acid (GABA), further protecting against central nervous system fatigue.48
Corticolimbic Inhibition and the Eradication of Evening Hyperphagia
Perhaps the most profound impact of the 30-gram breakfast anchor is its ability to influence late-day behavioral choices through direct central nervous system modulation. Extensive clinical research, pioneered by Leidy et al., has utilized advanced functional magnetic resonance imaging (fMRI) to evaluate the impact of a high-protein breakfast on the brain’s hedonic reward centers.45
In highly controlled randomized crossover trials, overweight and obese adolescents who habitually skipped breakfast were assessed over multiple weeks. They were assigned to either continue skipping breakfast, consume a normal-protein cereal-based breakfast (13g of protein), or consume a high-protein egg-and-beef-based breakfast (35g of protein). The meals were strictly isocaloric, containing exactly 350 kilocalories, and matched for fat and fiber to isolate the effect of the protein content.46 Predinner fMRI scans—conducted many hours after the morning meal had been fully digested—revealed remarkable neurological alterations. The high-protein breakfast uniquely and robustly suppressed neural activation in corticolimbic regions responsible for food motivation and reward-driven eating, specifically reducing blood-oxygen-level-dependent (BOLD) signals in the amygdala, hippocampus, and parahippocampus when subjects were exposed to visual food cues.47
The downstream behavioral consequence of this sustained neural suppression is a dramatic reduction in evening hyperphagia. Participants who consumed the high-protein breakfast exhibited a significant, measurable decline in ad libitum evening snacking on high-fat, high-sugar, energy-dense foods compared to those who skipped breakfast or consumed the normal-protein meal.46 By anchoring the day with 30 grams of protein, individuals preemptively dismantle the neurobiological drive that typically leads to catastrophic dietary non-compliance in the evening hours, effectively neutralizing cravings long before they materialize.
The Implementation of Protein Distribution: Frequency vs. Bolus Concentration
Skeletal muscle is a highly dynamic tissue existing in a constant state of flux, characterized by simultaneous periods of muscle protein breakdown (MPB) and muscle protein synthesis (MPS).60 The net accretion or retention of skeletal muscle mass relies entirely on achieving a positive net protein balance, where the rate of MPS exceeds the rate of MPB over a 24-hour period. Dietary amino acids, particularly the essential amino acid leucine, serve as both the structural building blocks for new tissue and the primary signaling molecules that activate the mechanistic target of rapamycin complex 1 (mTORC1), the master regulatory kinase governing MPS.61
The Optimization Strategy: Distribution Over Concentration
For maximum optimization of the hypertrophic response, a prevailing strategy in sports nutrition emphasizes the concept of “Distribution over Concentration.” Extensive research suggests that spreading total daily protein intake evenly across 3 to 4 discrete meals is a superior strategy for maximizing skeletal muscle protein synthesis compared to consuming the exact same daily quantity of protein in a single, massive daily meal.64
This optimization strategy is rooted in the “muscle full” concept. Historically, acute tracer studies indicated that the cellular machinery of human skeletal muscle is exceptionally responsive to a specific threshold of amino acids, maximizing its synthetic rate following the ingestion of approximately 20 to 30 grams of high-quality protein (which provides the requisite 2.5 to 3 grams of leucine to trigger mTORC1).3 By distributing protein intake into roughly four feedings of 0.40 to 0.55 grams per kilogram of body weight per meal, an individual can repeatedly stimulate the MPS response, creating multiple, overlapping peaks of anabolism throughout the day.3 Therefore, for individuals seeking the absolute pinnacle of muscle growth and recovery, adopting a 3 to 4 meal distribution strategy remains the clinically superior implementation.
Reconciling the Saturable Dose Hypothesis with Prolonged Kinetics
However, while multiple meals are optimal for generating frequent peaks of MPS, a recent paradigm shift in nutritional science has completely debunked the archaic corollary that “excess” protein consumed in a single large bolus is simply oxidized and wasted. The previous dogma assumed a strict physiological ceiling, positing that any protein ingested beyond the 30-gram threshold was irreversibly shunted toward hepatic oxidation, deamination, and urea excretion, offering zero anabolic benefit.3
This “anabolic ceiling” has been thoroughly disproven by landmark empirical research. A 2023 study by Trommelen et al., published in Cell Reports Medicine, utilized a highly sophisticated quadruple isotope tracer feeding-infusion methodology to track amino acid kinetics over an unprecedented 12-hour postprandial window following full-body resistance exercise.68 Human subjects consumed either 0g, 25g, or a massive 100g bolus of isotope-labeled milk protein. Earlier research designs were fundamentally flawed by their brevity; they typically terminated observation after only 4 to 6 hours.66
By extending the observation window to 12 hours, Trommelen et al. revealed that the human digestive and anabolic systems possess immense kinetic flexibility. The body does not waste the excess protein; rather, it drastically regulates the rate of gastric emptying and splanchnic release, slowing digestion to ensure a sustained, slow-drip release of amino acids into systemic circulation.66
The findings were definitive:
- The 100g protein bolus induced a significantly greater and more prolonged anabolic response than the 25g dose.68
- Plasma amino acid availability remained elevated for the entire 12-hour period in the 100g group, continuously driving subsequent incorporation into myofibrillar, connective, and plasma proteins with no sign of the anabolic curve flattening.68
- Whole-body protein net balance and mixed-muscle fractional synthetic rates increased in a dose-responsive manner, with no apparent upper limit.68
- While absolute amino acid oxidation increased slightly with the massive 100g dose, it represented a minimal fraction of the ingested load (less than 15%); the vast majority of the amino acids were successfully sequestered for tissue building.69
Therefore, a synthesis of the current evidence dictates the following protocol: To achieve the theoretical maximum of muscle protein synthesis, the “Distribution over Concentration” model (spreading protein across 3-4 meals) is the superior, optimized choice. However, from a practical and lifestyle-adherence perspective, the Trommelen data grants absolute dietary flexibility. Populations practicing time-restricted eating (intermittent fasting) or those who prefer fewer, larger meals are not severely compromising their lean mass; a single massive protein feeding (e.g., 80-100g) will safely sustain muscle repair and synthesis for an exponentially longer duration than a smaller feeding without being metabolically wasted.66
Defining Individualized Protein Targets: Lean Mass and Clinical Optimization
The establishment of an optimal daily protein target requires a stark departure from outdated baseline recommendations. The traditional Recommended Dietary Allowance (RDA) for the general population is set at a modest 0.8 grams of protein per kilogram of total body weight per day.75 However, this archaic figure was derived from short-term nitrogen balance studies intended merely to define the absolute minimum intake required to prevent clinical deficiency and overt muscle wasting in sedentary populations.77 It unequivocally does not represent an optimal intake for physical performance, body composition improvement, healthy aging, or metabolic regulation.77
Current sports science and clinical nutrition data strongly dictate higher thresholds. For sedentary individuals aiming for general health and the prevention of age-related sarcopenia, 1.2 to 1.5 g/kg of body weight is widely advisable.76 For active populations seeking to maximize muscle hypertrophy and adaptation, a robust range of 1.6 to 2.2 g/kg of body weight is required.18
Calculate Your Target: The Fat-Free Mass (FFM) Floor
A significant clinical limitation of standard body-weight-based calculations is their massive inaccuracy in specific morphological populations, notably individuals with clinical obesity or those with exceptionally high levels of muscularity. Because adipose tissue is metabolically inert regarding protein turnover, applying a standard formula (e.g., 2.0 g/kg) to the gross body weight of a severely obese individual results in a vastly overestimated, unpalatable, and unfeasible protein target.76 Conversely, utilizing standard baseline formulas on highly muscular athletes will underestimate their significantly elevated physiological turnover demands.82
To rectify this discrepancy and achieve true nutritional precision, optimal protein floors must be calculated based on Lean Body Mass (LBM) or Fat-Free Mass (FFM) rather than total gross body weight.83 Because protein requirements are intrinsically linked to the quantity of metabolically active tissue, determining targets via FFM provides a highly precise, individualized physiological baseline.85 We highly recommend that individuals use our Macro Calculator to determine their specific protein floor based precisely on their lean mass, ensuring absolute accuracy regardless of their current body fat percentage.
Clinical consensus identifies that the sheer maintenance of FFM requires approximately 1.5 to 1.9 grams of protein per kilogram of FFM daily, even in non-athletic older populations attempting weight loss.79
For athletic populations undergoing aggressive caloric restriction—such as physique athletes attempting to reduce body fat to extreme lows while preserving every ounce of lean tissue—the demand for dietary amino acids skyrockets. During severe energy deficits, a significantly greater proportion of amino acids is diverted toward hepatic gluconeogenesis to maintain systemic blood glucose, substantially increasing the risk of muscle catabolism. Extensive systematic reviews conducted by Helms et al. demonstrate that under conditions of intense resistance training combined with severe caloric restriction, the optimal protein target escalates drastically to 2.3 to 3.1 grams per kilogram of Fat-Free Mass (FFM) per day.82 Scaling the absolute protein intake upwards as leanness increases and caloric deficits deepen is paramount for preventing the loss of functional contractile tissue.89
| Population / Context | Standard Body Weight Calculation | Fat-Free Mass (FFM) Calculation |
| Sedentary / Healthy Aging | 1.0 – 1.2 g/kg | 1.5 g/kg FFM |
| Active / Hypertrophy Phase | 1.6 – 2.2 g/kg | 2.0 – 2.5 g/kg FFM |
| Severe Caloric Deficit / Athletes | 2.4 – 3.0 g/kg | 2.3 – 3.1 g/kg FFM |
Long-Term Adherence and Renal Safety Profiles
As the clinical prescription of high-protein diets scales upward to these optimized FFM targets, concerns regarding long-term renal safety frequently arise. The assertion that high protein intake damages human kidneys is a clinical extrapolation derived from patients with pre-existing Chronic Kidney Disease (CKD), in whom dietary protein restriction is absolutely medically necessary to prevent the accumulation of uremic toxins and slow the progression of renal failure.91
However, in individuals with healthy, highly functioning kidneys, there is no empirical evidence that a high-protein diet induces de novo renal pathology.8 A high-protein load does predictably increase the glomerular filtration rate (GFR), a phenomenon known as hyperfiltration. However, this represents a normal, reversible physiological adaptation required to clear increased nitrogenous waste, functionally analogous to how skeletal muscle hypertrophies in response to resistance training or how cardiac output increases during aerobic exercise.92
Robust meta-analyses of long-term randomized controlled trials extending beyond 12 to 24 months consistently demonstrate that while high-protein diets do initiate hyperfiltration and increase GFR, they do not negatively alter plasma creatinine levels or urinary albumin excretion—the true clinical markers of actual structural renal damage—in healthy adults.94 Therefore, high protein targets calculated from FFM are firmly established as both highly efficacious for body composition and medically safe for non-nephropathic populations over the long term.
Synthesis and Clinical Implications
Dietary protein acts as a profound metabolic fulcrum, shifting human physiology toward states of drastically increased energy expenditure, heightened neuroendocrine satiation, and optimal lean tissue retention. The assertion that the body severely struggles to store protein as fat is unequivocally supported by the complex stoichiometry of de novo lipogenesis; the biochemical conversion of amino acids to palmitate is a process that demands extreme inputs of ATP and NADPH, dissipating vast amounts of potential energy as heat. This metabolic reality, combined with the inherently high Thermic Effect of Food (TEF) characteristic of protein digestion, dictates that a caloric surplus driven primarily by protein does not result in the proportional adipose tissue accumulation universally observed with equivalent carbohydrate or fat surpluses.
Furthermore, protein serves as the paramount macro-intervention for behavioral dietary compliance. By agonizing specific apical receptors (PepT1, CaSR, GPRC6A) located in enteroendocrine L-cells, the ingestion of protein strongly stimulates the systemic release of the anorexigenic hormones GLP-1 and PYY while simultaneously suppressing the gastric secretion of the orexigenic hormone Ghrelin. Implementing the 30-gram breakfast anchor effectively exploits these exact neuroendocrine mechanisms. This simple intervention stabilizes diurnal glycemic variability, preserves the cortisol awakening response, and robustly silences corticolimbic reward centers in the brain, thereby preventing the afternoon energetic slump and systematically eliminating the neurological drive for evening hyperphagia.
Finally, the paradigms dictating protein meal distribution have been refined. To achieve the absolute superior optimization of muscle protein synthesis, spreading protein intake across 3 to 4 distinct meals maximizes the frequency of anabolic signaling. Yet, the archaic fear that large single boluses of protein are metabolically wasted has been definitively debunked; the gastrointestinal and anabolic machinery possesses immense kinetic flexibility, capable of safely sequestering and utilizing massive protein boluses (up to 100g) over a prolonged 12-hour postprandial window to sustain muscle protein synthesis. By adhering to precise, individualized Fat-Free Mass-based targets—utilizing tools like our Macro Calculator to find a specific protein floor—individuals can safely, sustainably, and effectively optimize their metabolic health, lean tissue retention, and long-term body composition without fear of renal detriment or metabolic inefficiency.
Works cited
- Thermic effect of food (TEF): How diet, lifestyle, and supplements may provide benefits., accessed June 3, 2026, https://examine.com/outcomes/thermic-effect-of-food/
- Thermic effect of a meal and appetite in adults: an individual participant data meta-analysis of meal-test trials – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC3873760/
- How much protein can the body use in a single meal for muscle-building? Implications for daily protein distribution – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5828430/
- Common questions and misconceptions about protein supplementation: what does the scientific evidence really show? – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11022925/
- Journal of Exercise Physiologyonline, accessed June 3, 2026, https://www.asep.org/asep/asep/JEPonlineFEBRUARY2022_Jose%20Antonio.pdf
- Dietary Protein and Energy Balance in Relation to Obesity and Co-morbidities – PMC – NIH, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC6087750/
- Thermic effect of feeding carbohydrate, fat, protein and mixed meal in lean and obese subjects – PubMed, accessed June 3, 2026, https://pubmed.ncbi.nlm.nih.gov/4025189/
- Clinical Evidence and Mechanisms of High-Protein Diet-Induced Weight Loss, accessed June 3, 2026, https://www.jomes.org/journal/view.html?doi=10.7570/jomes20028
- Clinical Evidence and Mechanisms of High-Protein Diet-Induced Weight Loss – PMC – NIH, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC7539343/
- The Influence of Physical Exercise, Ketogenic Diet, and Time-Restricted Eating on De Novo Lipogenesis: A Narrative Review – MDPI, accessed June 3, 2026, https://www.mdpi.com/2072-6643/17/4/663
- Regulation and Metabolic Significance of De Novo Lipogenesis in Adipose Tissues – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC6213738/
- De novo lipogenesis in metabolic homeostasis: More friend than foe? – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC4421107/
- Revisiting the concepts of de novo lipogenesis to understand the conversion of carbohydrates into fats: Stop overvaluing and extrapolating the renowned phrase “fat burns in the flame of carbohydrate” – PubMed, accessed June 3, 2026, https://pubmed.ncbi.nlm.nih.gov/39566326/
- Genetic control of de novo lipogenesis: role in diet-induced obesity – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC2874080/
- De novo lipogenesis in the liver in health and disease: more than just a shunting yard for glucose – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC4832395/
- De novo lipogenesis in humans: Metabolic and regulatory aspects – ResearchGate, accessed June 3, 2026, https://www.researchgate.net/publication/12932996_De_novo_lipogenesis_in_humans_Metabolic_and_regulatory_aspects
- Fatty acid synthesis – Wikipedia, accessed June 3, 2026, https://en.wikipedia.org/wiki/Fatty_acid_synthesis
- Optimal Protein Intake Guide & Calculator – Examine.com, accessed June 3, 2026, https://examine.com/guides/protein-intake/
- The cost of amino acid catabolism for energy utilization in broiler chickens – PMC – NIH, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC12051559/
- MIT Open Access Articles Reductive glutamine metabolism by IDH1 mediates lipogenesis under hypoxia, accessed June 3, 2026, https://dspace.mit.edu/server/api/core/bitstreams/4f820f04-5760-43c9-ac0a-4a899480c426/content
- Metabolic Complementation between Glucose and Amino Acid Drives Hepatic De Novo Lipogenesis and Steatosis | bioRxiv, accessed June 3, 2026, https://www.biorxiv.org/content/10.1101/2021.05.08.443229.full
- A randomized 3-way crossover study indicates that high-protein feeding induces de novo lipogenesis in healthy humans – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC6629161/
- A randomized 3-way crossover study indicates that high-protein feeding induces de novo lipogenesis in healthy humans – JCI Insight, accessed June 3, 2026, https://insight.jci.org/articles/view/124819/sd/1
- People Passionate about Starches Are Healthy and Beautiful – Dr. McDougall, accessed June 3, 2026, https://www.drmcdougall.com/education/information-all/people-passionate-about-starches-are-healthy-and-beautiful/
- Fat and carbohydrate overfeeding in humans: different effects on energy storage – PubMed, accessed June 3, 2026, https://pubmed.ncbi.nlm.nih.gov/7598063/
- The effects of consuming a high protein diet (4.4 g/kg/d) on body composition in resistance-trained individuals – PubMed, accessed June 3, 2026, https://pubmed.ncbi.nlm.nih.gov/24834017/
- The effects of consuming a high protein diet (4.4 g/kg/d) on body composition in resistance-trained individuals – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC4022420/
- The effects of consuming a high protein diet (4.4 g/kg/d) on body composition in resistance-trained individuals – Taylor & Francis, accessed June 3, 2026, https://www.tandfonline.com/doi/full/10.1186/1550-2783-11-19
- A high protein diet (3.4 g/kg/d) combined with a heavy resistance training program improves body composition in healthy – NSUWorks, accessed June 3, 2026, https://nsuworks.nova.edu/cgi/viewcontent.cgi?referer=&httpsredir=1&article=1030&context=hpd_hhp_facarticles
- The Effect of Peanut Butter Overfeeding in Trained Men and Women: A Pilot Trial, accessed June 3, 2026, https://www.journalofexerciseandnutrition.com/index.php/JEN/article/download/13/9/9
- The Effects of Overfeeding on Body Composition: The Role of Macronutrient Composition – A Narrative Review – ResearchGate, accessed June 3, 2026, https://www.researchgate.net/publication/322882933_The_Effects_of_Overfeeding_on_Body_Composition_The_Role_of_Macronutrient_Composition_-_A_Narrative_Review
- A high protein diet (3.4 g/kg/d) combined with a heavy resistance training program improves body composition in healthy trained men and women – a follow-up investigation – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC4617900/
- “Overfeeding and Body Composition” by Alex Leaf and Jose Antonio – TopSCHOLAR, accessed June 3, 2026, https://digitalcommons.wku.edu/ijes/vol10/iss8/16/
- The Effects of Overfeeding on Body Composition: The Role of Macronutrient Composition – A Narrative Review – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5786199/
- Physiology, Appetite And Weight Regulation – StatPearls – NCBI Bookshelf, accessed June 3, 2026, https://www.ncbi.nlm.nih.gov/books/NBK574539/
- The Sensory Mechanisms of Nutrient-Induced GLP-1 Secretion – MDPI, accessed June 3, 2026, https://www.mdpi.com/2218-1989/12/5/420
- Understanding the release mechanisms and secretion patterns for glucagon-like peptide-1 using the isolated perfused intestine as a model – Portland Press, accessed June 3, 2026, https://portlandpress.com/biochemsoctrans/article/53/01/135/235626/Understanding-the-release-mechanisms-and-secretion
- Proteins and Peptides from Food Sources with Effect on Satiety and Their Role as Anti-Obesity Agents: A Narrative Review – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11510221/
- Protein Digestion-Derived Peptides and the Peripheral Regulation of Food Intake – Frontiers, accessed June 3, 2026, https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2017.00085/full
- The L-Cell in Nutritional Sensing and the Regulation of Appetite – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC4507148/
- Proteins and Peptides from Food Sources with Effect on Satiety and Their Role as Anti-Obesity Agents: A Narrative Review – MDPI, accessed June 3, 2026, https://www.mdpi.com/2072-6643/16/20/3560
- The Science of Appetite Control: How Hormones Regulate Hunger and Satiety, accessed June 3, 2026, https://www.news-medical.net/health/The-Science-of-Appetite-Control-How-Hormones-Regulate-Hunger-and-Satiety.aspx
- Changes in ghrelin, GLP-1, and PYY levels after diet and exercise in obese individuals, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC10941879/
- High Protein Intake Stimulates Postprandial GLP1 and PYY Release – PMC – NIH, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC6548554/
- Eat a protein-rich breakfast to reduce food cravings, prevent overeating later, researcher finds | ScienceDaily, accessed June 3, 2026, https://www.sciencedaily.com/releases/2011/05/110519113024.htm
- Protein-rich breakfasts prevent unhealthy snacking in the evening – EurekAlert!, accessed June 3, 2026, https://www.eurekalert.org/news-releases/755690
- Beneficial effects of a higher-protein breakfast on the appetitive, hormonal, and neural signals controlling energy intake regulation in overweight/obese, “breakfast-skipping,” late-adolescent girls – PubMed, accessed June 3, 2026, https://pubmed.ncbi.nlm.nih.gov/23446906/
- High-Protein Breakfast Ideas for All-Day Energy | Nourishing Meals®, accessed June 3, 2026, https://nourishingmeals.com/2025/09/high-protein-breakfast-ideas-all-day-energy
- Study Details | NCT03134014 | High Protein Breakfast on Weight Management and Glycemic Control in ‘Breakfast-skipping’ Teens | ClinicalTrials.gov, accessed June 3, 2026, https://clinicaltrials.gov/study/NCT03134014
- Consuming high-protein breakfasts helps women maintain glucose control, study finds, accessed June 3, 2026, https://www.sciencedaily.com/releases/2014/04/140429162110.htm
- High-Protein Breakfast Helps Blood Sugar Control – Integrative Medicine of New Jersey, accessed June 3, 2026, http://integrativemedicineofnj.com/high-protein-breakfast-helps-blood-sugar-control
- Protein- and Calcium-Mediated GLP-1 Secretion: A Narrative Review – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC8634310/
- Fueling the Brain: Can Diet Overcome Neuro-Sleep Deficits? | Ubie Doctor’s Note, accessed June 3, 2026, https://ubiehealth.com/doctors-note/high-protein-breakfast-energy-fuel-brain-diet-47-n41e3
- A High-Protein Breakfast Induces Greater Insulin and Glucose-Dependent Insulinotropic Peptide Responses to a Subsequent Lunch Meal in Individuals With Type 2 Diabetes – PubMed, accessed June 3, 2026, https://pubmed.ncbi.nlm.nih.gov/25733459/
- High-Protein Breakfast Ideas | Fuel Your Morning | Scripps AMG, accessed June 3, 2026, https://scrippsamg.com/benefits-of-high-protein-breakfast/
- A randomized crossover, pilot study examining the effects of a normal protein vs. high protein breakfast on food cravings and reward signals in overweight/obese “breakfast skipping”, late-adolescent girls – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC4249715/
- Eat a protein-rich breakfast to reduce food cravings, prevent overeating later, researcher finds | EurekAlert!, accessed June 3, 2026, https://www.eurekalert.org/news-releases/804986
- Neural responses to visual food stimuli after a normal vs. higher protein breakfast in breakfast-skipping teens: a pilot fMRI study – PubMed, accessed June 3, 2026, https://pubmed.ncbi.nlm.nih.gov/21546927/
- Protein-rich breakfasts prevent unhealthy snacking in the evening – Medical Xpress, accessed June 3, 2026, https://medicalxpress.com/pdf283535433.pdf
- THE IMPACT OF PROTEIN QUANTITY, QUALITY, DISTRIBUTION, AND FOOD MATRIX ON MUSCLE PROTEIN SYNTHESIS – Gatorade Sports Science Institute, accessed June 3, 2026, https://www.gssiweb.org/sports-science-exchange/article/the-impact-of-protein-quantity–quality-distribution–and-food-matrix-on-muscleprotein-synthesis
- Meal Frequency and Nutrient Distribution: What is Ideal for Body Composition?, accessed June 3, 2026, https://symbiosisonlinepublishing.com/nutritionalhealth-foodscience/nutritionalhealth-foodscience15.php
- The anabolic response to protein ingestion during recovery from exercise has no upper limit in magnitude and duration in vivo in humans – Maastricht University, accessed June 3, 2026, https://cris.maastrichtuniversity.nl/en/publications/the-anabolic-response-to-protein-ingestion-during-recovery-from-e/
- Calculate Protein Intake | ATHLEAN-X, accessed June 3, 2026, https://learn.athleanx.com/calculators/protein-calculator
- accessed June 3, 2026, https://examine.com/faq/does-the-distribution-of-protein-intake-throughout-the-day-matter/#:~:text=Research%20suggests%20that%20distributing%20protein,distributed%20across%204%20meals%20daily.
- Does the distribution of protein intake throughout the day matter? – Examine, accessed June 3, 2026, https://examine.com/faq/does-the-distribution-of-protein-intake-throughout-the-day-matter/
- Rethinking protein intake needs – MySportScience, accessed June 3, 2026, https://www.mysportscience.com/post/rethinking-protein-intake-needs
- Protein Distribution and Muscle-Related Outcomes: Does the Evidence Support the Concept? – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC7285146/
- The anabolic response to protein ingestion during recovery from exercise has no upper limit in magnitude and duration in vivo in humans – PubMed, accessed June 3, 2026, https://pubmed.ncbi.nlm.nih.gov/38118410/
- 100g Protein in One Meal: What a 12-Hour Study Found — FitChef, accessed June 3, 2026, https://fitchef.com/studies/100g-protein-one-meal-study/
- 30g Protein Myth Debunked: They Stopped Watching Too Early, accessed June 3, 2026, https://fitchef.com/shorts/30g-protein-myth-they-stopped-watching/
- The Boundless Anabolic Response to Protein Post-Exercise – Healthspan, accessed June 3, 2026, https://www.gethealthspan.com/research/article/boundless-anabolic-response-protein-post-exercise
- The Anabolic Response to Protein Ingestion During Recovery From Exercise Has No Upper Limit in Magnitude and Duration In Vivo in Humans: A Commentary in, accessed June 3, 2026, https://journals.humankinetics.com/view/journals/ijsnem/34/5/article-p322.xml
- How Much Protein Can You Really “Use” From a Single Meal? – MASS Research Review, accessed June 3, 2026, https://massresearchreview.com/2025/06/27/how-much-protein-can-you-really-use-from-a-single-meal/
- Do you need 4 meals per day for maximum growth after all? – Menno Henselmans, accessed June 3, 2026, https://mennohenselmans.com/meal-frequency-science/
- accessed June 3, 2026, https://www.health.harvard.edu/blog/how-much-protein-do-you-need-every-day-201506188096#:~:text=How%20much%20protein%20do%20I,or%200.36%20grams%20per%20pound.
- Are you getting too much protein – Mayo Clinic Health System, accessed June 3, 2026, https://www.mayoclinichealthsystem.org/hometown-health/speaking-of-health/are-you-getting-too-much-protein
- How much protein do you need every day? – Harvard Health, accessed June 3, 2026, https://www.health.harvard.edu/blog/how-much-protein-do-you-need-every-day-201506188096
- How much protein should we really be eating? Five things to know – Stanford Medicine, accessed June 3, 2026, https://med.stanford.edu/news/insights/2026/03/how-much-protein.html
- Dietary protein content for an optimal diet: a clinical view – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5476844/
- How much protein do I need? A dietitian answers | UT MD Anderson, accessed June 3, 2026, https://www.mdanderson.org/cancerwise/how-much-protein-do-i-need-a-dietitian-answers.h00-159781179.html
- Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group, accessed June 3, 2026, https://www.espen.org/files/PIIS0261561414001113.pdf
- Proper Protein Intakes for Athletes – Dexalytics.com, accessed June 3, 2026, https://www.dexalytics.com/news/proper-protein-intakes-athletes/
- Calculation of protein requirements; a comparison of calculations based on bodyweight and fat free mass – PubMed, accessed June 3, 2026, https://pubmed.ncbi.nlm.nih.gov/35331517/
- Inadequacy of Body Weight-Based Recommendations for Individual Protein Intake—Lessons from Body Composition Analysis – MDPI, accessed June 3, 2026, https://www.mdpi.com/2072-6643/9/1/23
- Protein requirement in obesity – Amsterdam UMC, accessed June 3, 2026, https://pure.amsterdamumc.nl/ws/portalfiles/portal/142148308/Protein-requirement-in-obesity.pdf
- Inadequacy of Body Weight-Based Recommendations for Individual Protein Intake—Lessons from Body Composition Analysis – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5295067/
- Sarcopenia, Muscle Mass and Protein Intake in Adults Older Than 65 Years After Earlier Bariatric Surgery – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC12138283/
- accessed June 3, 2026, https://www.researchgate.net/publication/257350851_A_Systematic_Review_of_Dietary_Protein_During_Caloric_Restriction_in_Resistance_Trained_Lean_Athletes_A_Case_for_Higher_Intakes#:~:text=In%202014%2C%20the%20team%20led,content%20and%20leanness.%20…
- A Systematic Review of Dietary Protein During Caloric Restriction in Resistance Trained Lean Athletes: A Case for Higher Intakes – ResearchGate, accessed June 3, 2026, https://www.researchgate.net/publication/257350851_A_Systematic_Review_of_Dietary_Protein_During_Caloric_Restriction_in_Resistance_Trained_Lean_Athletes_A_Case_for_Higher_Intakes
- A systematic review of dietary protein during caloric restriction in resistance trained lean athletes: a case for higher intakes – PubMed, accessed June 3, 2026, https://pubmed.ncbi.nlm.nih.gov/24092765/
- Long-Term Effects of High-Protein Diets on Renal Function – PubMed, accessed June 3, 2026, https://pubmed.ncbi.nlm.nih.gov/28637384/
- Nutrition in Chronic Kidney Disease—The Role of Proteins and Specific Diets – MDPI, accessed June 3, 2026, https://www.mdpi.com/2072-6643/13/3/956
- High-protein diets: Are they safe? – Mayo Clinic, accessed June 3, 2026, https://www.mayoclinic.org/healthy-lifestyle/nutrition-and-healthy-eating/expert-answers/high-protein-diets/faq-20058207
- Higher Protein Intake Is Not Associated with Decreased Kidney Function in Pre-Diabetic Older Adults Following a One-Year Intervention—A Preview Sub-Study – MDPI, accessed June 3, 2026, https://www.mdpi.com/2072-6643/10/1/54
- The Effects of High-Protein Diets on Kidney Health and Longevity – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC7460905/
- Dietary Protein Intake and Chronic Kidney Disease – PMC, accessed June 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5962279/
**Reference:** *Leidy, H. J., et al. (2015). The role of protein in weight loss and maintenance. The American Journal of Clinical Nutrition.*