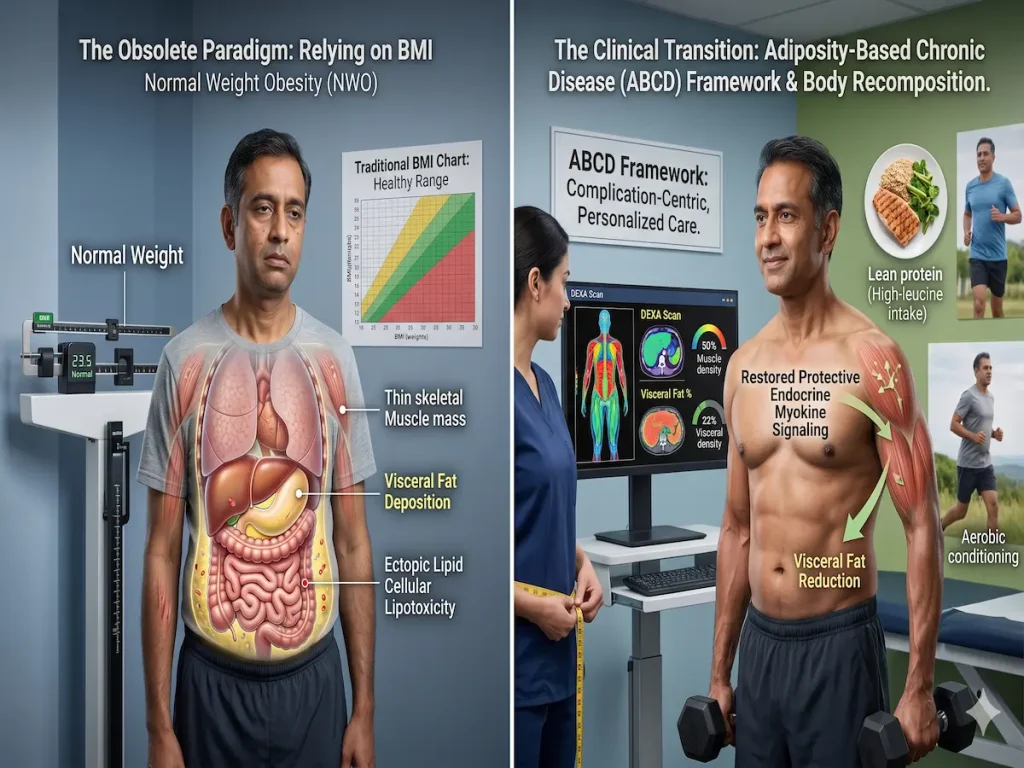
BMI is a population-level tool, not a diagnostic one. A person can have a “Normal” BMI (18.5–24.9) yet possess high levels of internal fat—a condition clinically known as Normal Weight Obesity or TOFI (Thin on the Outside, Fat on the Inside).
The Danger of Visceral Fat
Unlike subcutaneous fat (the kind you can pinch), visceral fat acts as an active endocrine organ. It secretes inflammatory cytokines directly into the portal vein, reaching the liver and interfering with insulin signaling. This is why TOFI individuals often have blood markers (glucose, lipids) similar to those with clinical obesity.
The Data-Driven Solution
1. The WHtR Metric: Research in The Lancet suggests that Waist-to-Height Ratio (WHtR) is a better predictor of lifespan than BMI. Aim for a WHtR of <0.50. Check yours now with the [Waist-Height Calculator](/waist-height-calculator/).
2. The Anabolic Push: Resistance training is non-negotiable. Muscle is metabolically active tissue that improves glucose disposal.
3. Protein Leverage: The body will continue to signal hunger until protein needs are met. Aim for 1.6g to 2.2g of protein per kg of body weight to shift your composition.
Normal Weight Obesity and Adiposity-Based Chronic Disease: Pathophysiology, Diagnostics, and Clinical Management
Introduction: The Global Adiposity Crisis and the Paradigm Shift in Diagnosis
For decades, the global medical community, guided by institutions such as the World Health Organization (WHO), has relied upon generalized anthropometric measurements to track and diagnose the burgeoning epidemic of metabolic dysfunction. The scale of this crisis is staggering; epidemiological data indicates that worldwide adult obesity has more than doubled since 1990, while adolescent obesity has quadrupled. By the year 2022, an estimated 2.5 billion adults—comprising 43% of the global adult population—were classified as overweight, with 890 million of these individuals living with clinical obesity. This global expansion is largely driven by complex, overlapping factors including shifting neurobiology, industrialized food systems, socioeconomic disparities, and increasingly obesogenic environments. The resultant economic burden is profound, with obesity estimated to add $3,559 annually (adjusted to 2012 dollars) to per-patient medical expenditures, encompassing increased costs in inpatient services, outpatient care, and prescription pharmacotherapy.
Historically, the clinical diagnosis of these conditions has been fundamentally intertwined with the Body Mass Index (BMI), an algorithmic surrogate marker calculated as weight in kilograms divided by height in meters squared. Under these traditional parameters, an individual is classified as overweight at a BMI of 25.0 to 29.9 kg/m2, and obese at a BMI of 30.0 kg/m2 or higher. However, an emerging consensus across the disciplines of endocrinology, cardiology, and metabolic research indicates that BMI is fundamentally limited, and its ubiquitous application obscures a highly prevalent, biologically insidious metabolic phenotype: Normal Weight Obesity (NWO).
Individuals presenting with Normal Weight Obesity maintain a statistically “healthy” BMI (typically between 18.5 and 24.9 kg/m2) but concurrently possess an abnormally high body fat percentage, frequently localized within the visceral anatomical compartment. Despite their outwardly normative physical appearance and compliant scale weight, these individuals exhibit severe metabolic dysregulation, systemic meta-inflammation, and elevated cardiometabolic mortality risks that parallel, or even exceed, those of individuals diagnosed with overt obesity.
Recognizing the inherent failures of weight-centric diagnostics, leading medical organizations, notably the American Association of Clinical Endocrinology (AACE), have spearheaded a comprehensive transition toward person-centered, complication-centric care. This modern paradigm formally adopts the framework of Adiposity-Based Chronic Disease (ABCD), which reframes obesity not as a static metric of excessive weight, but as a heterogeneous, progressive neuroendocrine disease characterized by excess, dysfunctional, and abnormally distributed adipose tissue. This report delivers an exhaustive analysis of Normal Weight Obesity and Adiposity-Based Chronic Disease, comprehensively exploring the mechanisms of adipose tissue biology, cellular lipotoxicity, myokine-adipokine crosstalk, advanced diagnostic methodologies, and evidence-based clinical interventions for body recomposition.
The Inherent Fallacy of the Body Mass Index Surrogate
The continued use of BMI as the primary threshold for clinical intervention generates substantial diagnostic errors, precipitating the misclassification of both metabolically healthy and metabolically compromised individuals. BMI was originally conceptualized as a population-level statistical tool rather than an individualized diagnostic instrument, and its inability to differentiate specific tissue compartments represents its most critical failing.
Failure to Differentiate Anatomical Tissue Compartments
The mathematical calculation of BMI strictly incorporates total mass and height, rendering it entirely blind to the distinct functional compartments of the human body: skeletal muscle mass, adipose tissue mass, bone mineral density, and total body water. Consequently, individuals with high degrees of fat-free mass, such as muscular athletes, are frequently misclassified into overweight or obese categories despite possessing exceptionally low levels of systemic adiposity. Conversely, and much more dangerously, older adults who have experienced profound age-related muscle loss (sarcopenia) routinely present with a “normal” BMI, despite carrying life-threatening levels of visceral adipose tissue.
When BMI is compared directly to reference standard measurement tools like dual-energy X-ray absorptiometry (DEXA), the degree of variability is striking. Research evaluating the prediction of true body fat percentage (%BF) from BMI reveals that the metabolic syndrome threshold for women often occurs at approximately 30% body fat, an adiposity level that frequently corresponds to a completely normal BMI. For men, metabolic syndrome equivalence to “overweight” can occur at 25% body fat, highlighting the critical necessity of using more direct measures of adiposity to manage disease risk.
Confounding Variables: Age, Sex, and Racial Disparities
BMI accuracy is heavily confounded by demographic variables, rendering universal charts clinically hazardous. Women inherently carry higher body fat percentages than men at equivalent BMIs due to reproductive biology, and the aging process naturally shifts overall body composition toward higher adiposity and lower muscle mass without necessarily altering total body weight. Most critically, BMI thresholds completely fail to accommodate distinct racial and ethnic phenotypes regarding lipid storage capacity and fat distribution.
Analyses of the National Health and Nutrition Examination Survey (NHANES) data from 2011 to 2018 demonstrate profound racial and ethnic discrepancies in body fat percentage at identical BMI levels. Studies show that Non-Hispanic Black individuals consistently demonstrate the lowest levels of predicted body fat percentage at specific BMI thresholds, whereas Non-Hispanic White individuals, particularly in advanced age cohorts (e.g., age 70), exhibit the highest predicted body fat levels at identical BMIs.
The disparities are exceptionally stark within Asian populations. Individuals of South Asian and East Asian descent routinely exhibit smaller skeletal frames and differ drastically in regional fat distribution compared to individuals of European descent. Asian populations demonstrate a highly accelerated accumulation of visceral and ectopic fat, precipitating the development of type 2 diabetes and cardiovascular disease at considerably lower BMIs. A failure to adjust for these racial and ethnic phenotypes results in systemic misdiagnosis, delayed clinical intervention, and occasionally the imposition of unjustified life insurance premium penalties for muscular demographics mislabeled as obese.
Defining Normal Weight Obesity and Adiposity-Based Chronic Disease
To address the expansive diagnostic gap left by BMI, researchers and clinical endocrinologists have formalized parameters to identify individuals who are metabolically compromised but maintain a normal weight.
Diagnostic Parameters and Mortality Risks of Normal Weight Obesity
Normal Weight Obesity is defined diagnostically by the combination of a normative BMI (18.5 to 24.9 kg/m2) existing alongside a body fat percentage that exceeds established healthy clinical thresholds. While exact normative body fat cutoffs fluctuate slightly based on specific clinical consensus guidelines, robust epidemiological studies, including extensive analyses of the Third National Health and Nutrition Examination Survey (NHANES III), have successfully classified NWO utilizing sex-specific upper tertiles of body fat. In these rigorous classifications, NWO is defined by a body fat percentage exceeding 23.1% in men and 33.3% in women.
The clinical consequences of remaining in a state of Normal Weight Obesity are severe and life-limiting. Data extracted from the NHANES III mortality study indicates that subjects presenting with NWO experience a four-fold higher prevalence of metabolic syndrome compared to normal-weight individuals with low body fat (16.6% versus 4.8%, respectively). Individuals with NWO demonstrate a significantly higher prevalence of dyslipidemia, hypertension (particularly in men), and established cardiovascular disease (particularly in women). Upon adjusting for systemic confounding variables, women with NWO demonstrate a statistically significant 2.2-fold increased risk for cardiovascular mortality compared to the low body fat control group.
When central obesity—characterized by visceral adiposity and measured clinically by a high waist-to-hip ratio (WHR) or waist-to-height ratio (WtHR)—is present alongside a normal BMI, the mortality risk escalates dramatically. The Mayo Clinic reports that subjects possessing a normal BMI but demonstrating central obesity exhibit the absolute highest cardiovascular death risks among all body composition phenotypes. Expected survival estimates are consistently lower for those with normal-weight central obesity compared to individuals who are classified as clinically obese by BMI but lack central fat distribution, proving that fat location is far more lethal than total body weight. Indeed, a waist-to-height ratio exceeding 0.5 at a normal BMI is now considered a highly pragmatic clinical measure to identify elevated mortality risk for cardiometabolic disease.
The Adiposity-Based Chronic Disease (ABCD) Framework
To reframe obesity from a static anthropometric label into a biologically accurate reflection of progressive neuroendocrine pathology, the American Association of Clinical Endocrinology (AACE) introduced and expanded the Adiposity-Based Chronic Disease (ABCD) framework. This modern complication-centric model stages the disease based entirely on the presence, severity, and clinical impact of weight-related complications, rather than relying solely on the mass of the patient.
| Diagnostic Category | Anthropometric Component | Clinical Component (Complications) | Clinical Prevention/Treatment Phase |
|---|---|---|---|
| Normal Weight | BMI <25 kg/m2 (or <23 in specific ethnicities) | No obesity-related complications present | Primary Prevention |
| Overweight / Obesity Stage 0 | BMI 25.0–29.9 kg/m2 (Overweight) or ≥30.0 kg/m2 (Obesity) | No obesity-related complications present | Secondary Prevention |
| Obesity Stage 1 | BMI ≥25.0 kg/m2 | Presence of one or more mild-to-moderate obesity-related complications | Tertiary Treatment |
| Obesity Stage 2 | BMI ≥25.0 kg/m2 | Presence of at least one severe complication requiring significant weight loss | Tertiary Treatment |
Table 1: AACE Diagnostic Categories and Staging for Adiposity-Based Chronic Disease
By leveraging the ABCD framework, modern clinicians can systematically identify patients who may technically fall into lower anthropometric categories—such as those with NWO—but who require aggressive Stage 1 or Stage 2 tertiary interventions due to the undeniable presence of metabolic syndrome, prediabetes, or dyslipidemia. The ABCD diagnostic model explicitly mandates that clinicians look beyond the scale, recognizing that excess, dysfunctional, and abnormally distributed adipose tissue can drastically impair health independently of total body weight.
Pathophysiology of Adipose Tissue Dysfunction: Hypertrophy, Ectopic Fat, and Meta-Inflammation
The fundamental biological pathology driving the elevated cardiometabolic risk in Normal Weight Obesity is not the absolute macroscopic mass of the adipose tissue, but rather its localized distribution, its cellular behavior, and its subsequent endocrine dysfunction. Adipose tissue expansion involves complex, reciprocal processes encompassing enteric sensory-motor actions, peripheral hormonal signaling, and central neurologic pathways.
Visceral Adipose Tissue (VAT) versus Subcutaneous Adipose Tissue (SAT)
In a metabolically healthy, energy-balanced state, excess dietary caloric intake is safely stored in subcutaneous adipose tissue (SAT), which lies directly beneath the skin. Healthy SAT expands primarily via hyperplasia—the biological recruitment, proliferation, and differentiation of new adipocyte precursor cells, which creates new, small, highly insulin-sensitive fat cells capable of safely sequestering lipids.
However, in states of metabolically unhealthy obesity, including NWO, the inherent storage capacity of the subcutaneous depot becomes critically limited. When hyperplastic expansion fails, the existing adipocytes are forced to undergo extreme hypertrophic expansion (cellular inflation). Hypertrophic adipocytes suffer from severe mechanical stress, localized tissue hypoxia, and cellular necrosis. Once the SAT reaches its absolute storage limit, further caloric overload initiates “lipid overspill,” leading to the highly dangerous accumulation of fat in ectopic tissues—namely the visceral adipose depots within the abdominal cavity, the liver, the skeletal muscle, the pancreas, and the myocardium.
Visceral Adipose Tissue (VAT) behaves fundamentally differently than SAT. It is highly metabolically active, highly lipolytic, and functions as an aberrant, pathogenic endocrine organ. VAT is uniquely atherogenic, constantly releasing free fatty acids (FFAs) and pro-inflammatory cytokines into systemic circulation, thereby fostering a state of chronic, low-grade inflammation often termed “meta-inflammation”. In individuals maintaining a normal BMI, an elevated Visceral Fat Area (VFA)—often defined as exceeding 100 cm2—demonstrates an independent, nonlinear, positive association with incident metabolic syndrome.
Cross-sectional epidemiological investigations, such as data derived from 1250 participants in the Framingham Heart Study, clearly demonstrate the distinct dangers of visceral fat. While both SAT and VAT are positively related to basic inflammatory markers like C-reactive protein (CRP), fibrinogen, and interleukin-6 (IL-6), VAT is significantly more highly associated with specific markers of vascular damage and oxidative stress, namely urinary isoprostanes and monocyte chemoattractant protein-1 (MCP-1). The contribution of VAT to systemic inflammation and oxidative stress cannot be accounted for by clinical measures of BMI alone, confirming that visceral fat generates an independent pathogenic inflammatory milieu.
Animal Models of Adipose Tissue Inflammation
The cellular mechanics of adipose tissue dysfunction have been exhaustively documented in murine models. Studies utilizing high-fat diet (HFD) mouse models demonstrate that extreme adipocyte expansion leads directly to hepatic steatosis and systemic metabolic dysfunction. Specific immunological interactions dictate this process; for example, research indicates that eosinophils are required to sustain alternatively activated macrophages in adipose tissue, and mice lacking these eosinophils develop profound insulin resistance despite equivalent body fat accumulation. Furthermore, regulatory T cells (T-reg cells) highly enriched in lean abdominal fat are progressively lost in hypertrophic obesity, stripping the tissue of its anti-inflammatory defenses and triggering localized insulin resistance. This pathogenic signature is not limited to adults; DNA methylation modifications associated with maternal obesity are identifiable in the blood of newborn infants via heel stick analysis, proving that the metabolic consequences of adipose dysfunction span generations.
The Portal Vein Hypothesis and Cellular Lipotoxicity
The specific anatomical location of visceral fat makes it particularly devastating to hepatic and pancreatic function. The classical “Portal Vein Hypothesis” posits that because visceral adipose tissue depots drain directly into the portal venous system, the liver is subjected to a massive, unfiltered influx of free fatty acids and lipolytic cytokines released from dysfunctional visceral fat.
This direct, unrelenting portal exposure forces the liver to process excessive FFAs, rapidly driving the development of hepatic steatosis (non-alcoholic fatty liver disease). The accumulation of hepatic fat profoundly disrupts normal insulin clearance, rendering the liver severely insulin resistant and actively accelerating the pathogenesis of type 2 diabetes. While subsequent research has also highlighted the role of systemic free fatty acids derived from abdominal subcutaneous fat, the portal delivery of visceral adipocytokines remains a central pillar in the pathophysiology of metabolic syndrome.
Molecular Lipotoxicity: Diacylglycerols (DAGs) and Ceramides
The precise molecular mechanisms linking ectopic fat deposition to target-organ insulin resistance involve the intracellular accumulation of highly lipotoxic lipid intermediates, primarily diacylglycerols (DAGs) and ceramides. Under conditions of overnutrition and excessive VAT lipolysis, fatty acids flux relentlessly into the liver and skeletal muscle. While healthy cells neutralize excess lipid flux by safely packaging it into inert triglycerides within lipid droplets, pathological excess generates bioactive DAGs and ceramides.
In the liver, the pathological accumulation of sn−1,2-diacylglycerol strongly activates the ϵ isoform of protein kinase C (PKC$\epsilon$). Once activated, PKC$\epsilon$ phosphorylates the insulin receptor (INSR) specifically at the Thr1160 residue. This single phosphorylation event results in the near-total inhibition of the insulin receptor’s intrinsic tyrosine kinase activity, thereby blinding the liver to the presence of insulin. Consequently, all downstream arms of hepatocellular insulin signaling are disrupted: the liver fails to stimulate net glycogen synthesis, fails to upregulate de novo lipogenic genes, and crucially, fails to downregulate gluconeogenic genes. The result is unchecked hepatic glucose production, leading directly to fasting hyperglycemia.
A parallel mechanism occurs in skeletal muscle, the body’s primary sink for glucose disposal. In muscle tissue, intracellular DAG accumulation activates a different isoform, PKC$\theta$. This activation leads to the phosphorylation and inhibition of insulin receptor substrate-1 (IRS-1), effectively antagonizing insulin-mediated glucose uptake.
Simultaneously, ceramides and their derivatives accumulate in these metabolic organs alongside DAGs. Elevated ceramide species antagonize distinct nodes of the insulin signaling cascade and provoke severe localized tissue inflammation. Therefore, individuals presenting with Normal Weight Obesity, having surpassed their safe subcutaneous storage capacity, are actively poisoning their liver and skeletal muscle with DAGs and ceramides, precipitating severe clinical insulin resistance despite maintaining a normal BMI.
The Personal Fat Threshold Hypothesis and Ethnic Metabolic Disparities
The concepts of ectopic lipid deposition and lipotoxicity integrate perfectly into the “Personal Fat Threshold” hypothesis, a paradigm-shifting model proposed by Professor Roy Taylor to explain the etiology of type 2 diabetes across all body weights. This hypothesis resolves the long-standing clinical paradox of why certain individuals develop type 2 diabetes at a highly lean BMI of 22 kg/m2, while others remain remarkably insulin sensitive at a morbidly obese BMI of 35 kg/m2.
Individualized Capacity for Subcutaneous Storage
The Personal Fat Threshold hypothesis dictates that every individual possesses a unique, genetically determined maximal capacity to safely store fat within subcutaneous depots. If an individual exceeds this singular personal threshold—regardless of their absolute BMI—lipid overspill is initiated, driving fat directly into the liver and subsequently over-spilling into the pancreas. In the pancreas, this ectopic fat triggers cellular dedifferentiation and lipotoxicity within the β-cells, effectively “clogging” the biological machinery and switching off the specific genes required for glucose-stimulated insulin secretion.
Data drawn from the United Kingdom Prospective Diabetes Study (UKPDS) cohort, which forms the basis of much of our modern understanding of diabetes, reveals that one in three individuals diagnosed with type 2 diabetes in the 1970s and 1980s possessed a BMI of less than 25 kg/m2. Compelling modern metabolic trials have definitively proven that type 2 diabetes in these normal-weight individuals is driven by the exact same reversible pathophysiology as seen in obese individuals.
In highly controlled trials where individuals with established type 2 diabetes and a BMI <27 kg/m2 underwent repeated 5% weight loss cycles, researchers observed profound metabolic normalization. Following the targeted energy deficit, liver fat content plummeted from an average of 16.0% down to 3.1%, and hepatic fat export returned to normal normative ranges. As this concealed excess intra-hepatic and intra-pancreatic fat was cleared, pancreatic β-cell first-phase insulin response significantly recovered. This clearance resulted in sustained diabetes remission (defined as HbA1c <48 mmol/mol off all glucose-lowering agents) in 70% of the normal-weight cohort. These data unequivocally confirm the Personal Fat Threshold hypothesis: the etiology of type 2 diabetes does not depend on absolute BMI, but rather on crossing an individualized threshold of visceral lipotoxicity.
The South Asian Metabolic Phenotype
The clinical implications of the Personal Fat Threshold are most visibly and dangerously pronounced in specific ethnic populations, particularly among individuals of South Asian descent. South Asian Americans experience disproportionately high rates of atherosclerotic cardiovascular disease (ASCVD) and cardiometabolic dysfunction compared to virtually all other ethnic groups in the United States.
South Asian populations are genetically predisposed to abdominal obesity and possess a severely limited capacity for subcutaneous fat expansion. Consequently, they rapidly exceed their personal fat threshold, exhibiting significantly higher distributions of visceral fat, intermuscular fat, and intrahepatic fat at standard, globally accepted BMIs. Epidemiological data demonstrates that to capture the equivalent age- and sex-adjusted incidence of type 2 diabetes observed in Caucasian populations at a BMI of 30.0 kg/m2, the equivalent BMI cutoff for South Asians must be drastically lowered, often to levels between 23.0 and 27.5 kg/m2.
Furthermore, data modeling the incidence of diabetes over a 12.8-year follow-up confirms that South Asian, Chinese, and Black ethnic subgroups develop metabolic complications at vastly different anthropometric thresholds than White populations. The inherent propensity for Asian demographics to rapidly exceed their personal fat threshold underscores the profound danger of normal weight obesity, necessitating aggressive, early screening for visceral adiposity using culturally adapted clinical guidelines.
Endocrine Crosstalk: Adipokines, Inflammation, and Myokines
The metabolic health of the human body is maintained by a highly complex, dynamic endocrine dialogue between adipose tissue, the liver, and skeletal muscle. These tissues function not merely as inert storage or mechanical structures, but as highly active endocrine organs responsible for secreting biologically active proteins known as adipokines, hepatokines, and myokines. In the context of Normal Weight Obesity, this delicate crosstalk is severely disrupted.
The Leptin/Adiponectin Axis
When visceral adipose tissue undergoes pathological hypertrophy, it drastically alters its secretory profile, shifting the systemic environment toward chronic inflammation. Two of the most critical adipokines regulating this process are leptin and adiponectin. Leptin is primarily produced by adipose tissue to regulate satiety and energy expenditure; however, in states of expanding adiposity, it is hyper-secreted, leading to a pathological state of systemic leptin resistance. Conversely, adiponectin, an adipokine possessing potent anti-inflammatory, anti-atherogenic, and insulin-sensitizing properties, is markedly downregulated in individuals suffering from visceral obesity and clinical insulin resistance.
The calculated Leptin/Adiponectin (L/A) ratio has consequently emerged as a highly sensitive, predictive biomarker for metabolic dysregulation. Clinical studies analyzing normal-weight individuals against non-diabetic obese individuals demonstrate that those with excess adiposity exhibit drastically elevated L/A ratios (8.21 versus 0.59 in healthy controls), correlating with severe underlying insulin resistance. Furthermore, dysfunctional visceral adipocytes secrete high volumes of tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), which directly infiltrate local tissues, interfere with cellular insulin signaling cascades, and promote systemic atherosclerosis. In type 2 diabetic patients, serum concentrations of C-reactive protein (CRP) and TNF-α are significantly correlated with waist circumference and body fat mass, highlighting the direct link between central adiposity and elevations in inflammatory cytokines.
Skeletal Muscle as an Endocrine Organ: Myokine Secretion
Just as dysfunctional fat secretes pathogenic adipokines, contracting skeletal muscle secretes highly protective proteins known as myokines. Myokines play a decisive role in regulating lipid metabolism, counteracting the lipotoxic effects of visceral fat, and orchestrating systemic energy balance.
Muscle-derived IL-6—which acts via entirely different pathways than the chronic, macrophage-derived IL-6 secreted by fat—stimulates active lipolysis and enhances fat oxidation through the activation of 5′-AMP-activated protein kinase (AMPK). Furthermore, exercise stimulates the cleavage of the FNDC5 gene, releasing the myokine Irisin into systemic circulation. Irisin possesses the extraordinary ability to induce the “browning” of white adipose tissue, a process that converts biologically inert, energy-storing white fat cells into mitochondria-rich, energy-dissipating brown fat cells.
Another critical myokine, muscle-derived IL-15, plays a direct role in regulating overall fat mass. Genetic studies involving IL-15 receptor alpha (IL-15R$\alpha$) polymorphisms, particularly in conjunction with MTHFR gene variants, show direct correlations with resting metabolic rate and the incidence of the Normal Weight Obese syndrome. Additionally, Brain-Derived Neurotrophic Factor (BDNF) and Fibroblast Growth Factor 21 (FGF21) regulate beta-oxidation and decrease lipogenesis within the liver, further protecting against hepatic steatosis.
However, myostatin, a myokine that negatively regulates muscle growth, becomes elevated in pro-inflammatory environments, sharing space with pro-inflammatory organokines like resistin and chemerin. In individuals with Normal Weight Obesity, who frequently suffer from low muscle mass and severe physical inactivity, the protective output of irisin, BDNF, and IL-15 is critically diminished. This loss of protective myokine signaling allows visceral adiposity and systemic meta-inflammation to proliferate unchecked, accelerating cardiovascular disease.
Sarcopenic Obesity and the Pathogenesis of Anabolic Resistance
A primary, yet often overlooked, driver of Normal Weight Obesity is the simultaneous, insidious loss of skeletal muscle mass paired with the covert accumulation of adipose tissue—a dual pathology formally recognized as Sarcopenic Obesity (SO). Because skeletal muscle tissue is highly dense, its gradual volumetric loss can easily mask the simultaneous gain of lighter adipose tissue, keeping the net weight and BMI completely stable on a scale while the patient’s body composition deteriorates drastically.
Diagnostic Criteria for Sarcopenia
The European Working Group on Sarcopenia in Older People (EWGSOP2) provides clinical consensus guidelines defining sarcopenia as a progressive muscular disease characterized by the presence of both low muscle quantity (mass) and low muscle function (strength or performance).
| Diagnostic Test / Metric | EWGSOP2 Sarcopenia Cut-off for Men | EWGSOP2 Sarcopenia Cut-off for Women |
|---|---|---|
| Grip Strength (Muscle Function) | <27 kg | <16 kg |
| Chair Stand Test (Performance) | >15 seconds for 5 rises | >15 seconds for 5 rises |
| Appendicular Skeletal Muscle (ASM) | <20 kg | <15 kg |
| ASM / height$^2$ | <7.0 kg/m2 | <5.5 kg/m2 |
| Gait Speed | ≤0.8 m/s | ≤0.8 m/s |
Table 2: EWGSOP2 Sarcopenia Cut-off Points for Low Muscle Quantity and Performance
To accurately capture the intersection of sarcopenia and obesity, diagnostic frameworks increasingly utilize combined indices. For example, the SARC-CalF questionnaire (which incorporates calf circumference) combined with Percentage of Body Fat (PBF) or Waist Circumference (WC) is utilized to identify at-risk populations. In men, severe sarcopenic obesity risk is identified at a SARC-CalF score ≥11 alongside a PBF ≥25% or a WC ≥90 cm; for women, the threshold is a SARC-CalF ≥11 with a PBF ≥35% or a WC ≥85 cm.
When clinical sarcopenia merges with elevated visceral adiposity, it creates a phenomenally dangerous synergistic phenotype. In Sarcopenic Obesity, the precipitous drop in muscle mass radically reduces total resting energy expenditure and diminishes the body’s primary sink for insulin-mediated glucose disposal, accelerating the severity of metabolic syndrome, physical frailty, and eventual mortality.
The Mechanics of Anabolic Resistance
Reversing the muscle loss inherent in Sarcopenic Obesity is biologically arduous due to a severe physiological barrier known as anabolic resistance. Anabolic resistance is defined as the blunted, diminished ability of skeletal muscle to stimulate muscle protein synthesis (MPS) in response to standard anabolic stimuli—namely, the ingestion of dietary amino acids and the mechanical load of resistance exercise.
While a degree of anabolic resistance is a recognized hallmark of the biological aging process, its severity is vastly accelerated by obesity, insulin resistance, systemic inflammation, and prolonged sedentary behaviors. Ectopic lipid accumulation within the muscle fibers themselves—a condition termed myosteatosis—directly impairs the mechanistic target of rapamycin (mTOR) signaling pathway, which operates as the master molecular regulator of muscle protein synthesis. Furthermore, age-related declines in endogenous hormones exacerbate this resistance. For instance, the drastic decrease in circulating estrogens during menopause removes critical protective signals that normally maintain muscle mass and prevent unfavorable central fat distribution in females.
Consequently, individuals suffering from Normal Weight Obesity and accompanying sarcopenia cannot successfully build or even maintain their muscle mass using the standard dietary protein guidelines deemed sufficient for healthy, active youth. They exist in a state of high catabolism and require highly targeted hyper-nutritional and intense mechanical interventions to forcefully overcome this entrenched signaling blockade.
Advanced Diagnostic Modalities for Body Composition Assessment
Because the BMI surrogate is demonstrably insufficient for diagnosing Normal Weight Obesity, modern healthcare providers and metabolic researchers must utilize specialized body composition measurement modalities to accurately delineate fat mass, lean mass, bone mineral content, and total body water. The selection of an appropriate diagnostic modality relies on balancing clinical accuracy, anatomical compartment specificity, technical feasibility, and economic cost.
Dual-Energy X-Ray Absorptiometry (DEXA)
Dual-Energy X-ray Absorptiometry (DEXA) is universally regarded as the clinical “gold standard” reference method for quantifying body composition. Originally designed for bone density testing, DEXA operates by passing two low-dose X-ray beams of differing energy levels through the body. Because adipose tissue, lean muscular tissue, and bone mineral attenuate these X-ray photons at distinctly different, predictable rates, the DEXA software can highly accurately calculate the mass of each specific compartment.
Crucially, DEXA provides detailed segmental analysis, allowing clinicians to independently evaluate the arms, legs, and trunk. This permits the precise quantification of visceral fat mass, a vital metric that is entirely impossible to extract from standard anthropometric scales. The clinical error margin for a DEXA scan is remarkably tight, ranging from merely ±0.5% to 2.0%. While it requires clinical-grade machinery, certified radiologic technicians, and incurs moderate costs per test ($45 to $400), its precision in identifying ectopic fat distribution makes it indispensable for diagnosing true Normal Weight Obesity.
Bioelectrical Impedance Analysis (BIA)
Bioelectrical Impedance Analysis (BIA) represents the most common clinical and consumer alternative to DEXA. BIA devices—ranging from advanced multi-frequency clinical platforms (e.g., InBody) to consumer smart scales—operate by transmitting a harmless, low-level electrical current through the patient’s body. The physical principle relies on the fact that lean skeletal muscle tissue is highly hydrated and conducts electricity efficiently, whereas adipose tissue is highly anhydrous and acts as a biological insulator. By measuring the electrical resistance and reactance across the body, BIA algorithms estimate total body water and extrapolate fat-free mass.
While highly convenient, completely non-invasive, and cost-effective ($30 to $300), BIA methodologies rely on strict physiological assumptions regarding constant total body hydration. A single glass of water, the timing of a recent meal, skin temperature, or a prior workout can significantly skew electrical impedance readings. Research analyzing commercial BIA scales against DEXA reference standards reveals that BIA models systematically underestimate true fat mass by approximately 2 to 4 kg, resulting in error margins ranging widely from ±3% to 10%. Furthermore, studies indicate that BIA tends to overestimate fat-free mass by as much as 3.38 to 8.28 kg in overweight populations, while simultaneously underestimating it in highly lean populations (BMI < 16). Despite these inherent limitations, modern segmental multi-frequency BIA (MF-BIA) has vastly improved accuracy regarding limb length disparities and remains a highly effective tool for tracking longitudinal, relative changes in a patient’s body composition, provided the individual rigidly controls for hydration variables before scanning.
To compensate for discrepancies between accessible tools like BIA or skinfold calipers and the gold-standard DEXA, researchers have developed specific linear regression adjustments. For example, to adjust basic bioimpedance fat percentage to a true DEXA-equivalent value, the established equation is: 10.947+(1.030×fat mass bioimpedance%). For skinfold anthropometry, the equation is: 3.362+(1.326×fat mass anthropometry%). These mathematical adjustments allow field researchers and clinicians without access to DEXA to secure highly objective body fat percentages.
Air Displacement Plethysmography (Bod Pod) and Hydrodensitometry
Hydrodensitometry (underwater weighing) and Air Displacement Plethysmography (ADP, commonly known as the Bod Pod) both operate on the principle of measuring total body density to deduce composition. In hydrodensitometry, the subject is completely submerged in water, and body volume is calculated based on water displacement and residual lung volume. In ADP, the patient sits inside a sealed, computerized chamber, and the device calculates body volume by measuring the exact volume of air displaced.
Once total body density is established, established algorithmic equations (e.g., the Siri or Brozek formulas) partition the weight into fat mass and fat-free mass. Both methods provide near-gold-standard accuracy (±1.5% to 3%) under perfect laboratory conditions. However, ADP accuracy can be easily disrupted by trapped air within loose clothing, excess facial hair, or even the wearing of lower-limb prostheses, requiring strict environmental controls to match DEXA precision. Additionally, body density formulas rely on generalized constants for the density of fat-free mass, which can vary slightly across different racial demographics and age cohorts.
Comparative Synthesis of Diagnostic Modalities
| Measurement Method | Core Mechanism of Action | Error Margin vs. DEXA | Clinical Utility & Target Compartments | Estimated Cost Per Test |
|---|---|---|---|---|
| DEXA Scan | Dual-energy X-ray attenuation | ±0.5–2.0% (Gold Standard) | Highly precise for bone density, visceral fat, segmental lean mass. | $45 – $400 |
| Hydrostatic Weighing | Water displacement (Body Density) | ±1.5–2.0% | Research-grade testing. Requires complete underwater submersion. | $50 – $150 |
| Bod Pod (ADP) | Air displacement (Body Density) | ±2.0–3.0% | Clinical/Lab alternative to DEXA. Quick, avoids radiation and water. | $50 – $150 |
| Skinfold Calipers | Anthropometric subcutaneous fold | ±3.5–5.0% | Highly dependent on technician skill. Cannot measure visceral fat. | $10 – $300 |
| BIA (Clinical/Consumer) | Electrical current resistance | ±3.0–10.0% | Estimates whole-body trends. Highly sensitive to systemic hydration. | $30 – $300 |
Table 3: Comprehensive Comparison of Body Composition Measurement Modalities
Beyond complex, high-cost machinery, pragmatic clinical anthropometric markers—specifically precise Waist Circumference (WC) and the Waist-to-Height Ratio (WtHR)—remain vital, low-cost, frontline screening tools in primary care. Given the lethality of central adiposity, a WtHR exceeding 0.5 at a normal BMI is universally recognized as a highly sensitive, immediate clinical indicator for elevated mortality risk linked to underlying cardiometabolic disease.
Clinical Management: Transitioning from Weight Loss to Body Recomposition
The traditional medical advice issued universally to overweight populations—to achieve a global, non-specific reduction in total body weight—is entirely counterproductive and biologically hazardous for individuals presenting with Normal Weight Obesity and Sarcopenic Obesity. Because their total macroscopic body mass already resides within a normative, statistically “healthy” range, aggressive, unmitigated global weight loss driven by severe caloric restriction will inevitably precipitate further catastrophic losses in critical skeletal muscle mass. This loss deepens the severity of sarcopenia, radically reduces basal metabolic rate, and severely exacerbates the underlying anabolic resistance, effectively creating a smaller, but vastly frailer and more metabolically damaged patient.
Consequently, the clinical treatment paradigm must pivot entirely away from arbitrary weight reduction and focus exclusively on body recomposition: the deliberate, simultaneous physiological process of reducing ectopic and visceral adipose tissue while aggressively maintaining, or hypertrophying, skeletal muscle mass. The essential pillars of a successful lifestyle medicine prescription for body recomposition encompass highly structured nutritional periodization, the mandatory implementation of progressive resistance training, and specific aerobic cardiovascular optimization.
Nutritional Interventions and Hyper-Protein Periodization
To biologically trigger lipolysis and clear ectopic fat stores residing in the liver, pancreas, and visceral cavity, a modest, controlled caloric deficit remains strictly required. Current lifestyle medicine guidelines advocate for an individualized dietary plan that achieves a calculated energy deficit of 500 to 750 kcal per day. This specific deficit range has been clinically demonstrated to safely and effectively reduce visceral fat area, lower circulating triglycerides, and induce the remission of metabolic syndrome without triggering extreme adaptive thermogenesis.
However, to definitively prevent the concurrent catabolism of lean muscle tissue during this sustained caloric deficit, dietary protein intake must be drastically upregulated beyond standard baseline recommendations. Dietary protein serves multiple vital functions: it provides the essential amino acid substrates required to fuel muscle protein synthesis, repairs mechanical micro-tears induced by progressive exercise, and provides a high degree of satiety to ensure dietary adherence.
To successfully penetrate and overcome the inherent anabolic resistance seen in NWO, sarcopenic, and aging populations, extensive clinical evidence and meta-analyses strongly support prescribing a daily protein intake ranging from 1.6 to 2.2 grams per kilogram of body weight (approximately 0.7 to 1.0 g per pound of body weight). High-quality protein sources that are exceptionally rich in the essential amino acid leucine (such as lean meats, whey isolate, and Greek yogurt) are absolutely vital, as leucine acts as the primary biological trigger for activating the mTOR signaling pathway. Furthermore, clinical supplementation with branched-chain amino acids (BCAAs), the leucine metabolite β-hydroxy-β-methylbutyrate (HMB), and omega-3 polyunsaturated fatty acids (n3-PUFA) can successfully potentiate the anabolic response to protein feeding in resistant older adults.
It is critical to note that alternative nutritional approaches utilizing aggressive, continuous caloric restriction without sufficient protein support—or highly restrictive dietary patterns like alkaline diets lacking adequate essential amino acids—consistently fail to induce favorable body recomposition, often worsening muscle loss despite superficial improvements in BMI. Instead, intermittent and progressive energy restrictions combined with high-protein refeeds demonstrate superior efficacy in preserving fat-free mass.
The Clinical Imperative of Resistance Training
Dietary intervention alone, regardless of protein optimization, cannot fully restore the vital endocrine myokine function lost to decades of physical inactivity. Progressive resistance training (RT) is a non-negotiable, foundational medical component for managing Adiposity-Based Chronic Disease, overcoming anabolic resistance, and reversing Sarcopenic Obesity.
Mechanical tension placed upon skeletal muscle acts as a profoundly potent, independent physiological stimulator of muscle protein synthesis, working synergistically with protein ingestion to force the reversal of the anabolic blockade. Meta-analyses of dozens of randomized controlled trials (encompassing nearly 74 specific RCTs) conclusively demonstrate that increasing daily protein ingestion combined with structured resistance training significantly enhances measurable gains in lean body mass, lower-body muscle strength, and functional test performance, even in highly resistant populations older than 65 years. Clinical guidelines explicitly dictate performing resistance exercises targeting all major muscle groups a minimum of 2 to 3 times per week.
Aerobic Exercise Protocols and Behavioral Lifestyle Medicine
Simultaneously, the active mitigation and oxidation of visceral adiposity require the establishment of a robust aerobic cardiovascular base. Current clinical lifestyle medicine guidelines prescribe a highly specific two-pronged approach: the active promotion of structured physical activity combined with the systematic reduction of daily sedentary time.
For structured cardiovascular conditioning, guidelines dictate the completion of 150 to 300 minutes of moderate-intensity aerobic exercise per week, or alternatively, 75 to 100 minutes of vigorous-intensity aerobic exercise. In precise clinical terms, moderate-intensity aerobic exercise (AE-M) is defined as achieving 45% to 65% of VO2max, or 65% to 75% of maximum heart rate (HRmax), sustained for sessions lasting 30 to 60 minutes, 3 to 5 times per week. Vigorous aerobic intervals, such as High-Intensity Interval Training (HIIT) involving intervals reaching 80% to 90% of heart rate reserve (HRR), demonstrate exceptional efficacy in rapidly depleting visceral fat stores and improving insulin sensitivity. This aerobic conditioning enhances cardiac stroke volume, massively upregulates mitochondrial density and oxidative enzymes within skeletal muscle, and actively accelerates the terminal oxidation of the free fatty acids released from lipolyzed visceral depots.
Beyond structured exercise regimens, behavioral therapy utilizing the “6A model” (Ask, Assess, Advise, Agree, Assist, Arrange) and cognitive-behavioral techniques are highly efficacious in ensuring long-term patient adherence. Reducing overall sedentary time by forcing the interruption of continuous sitting—recommending that patients stand up, stretch, or walk for at least 5 minutes every 30 to 60 minutes—is critical for maintaining postprandial insulin sensitivity and preventing lipid pooling. Furthermore, managing chronic psychological stress (which chronically elevates the highly lipogenic and catabolic hormone cortisol) and optimizing deep sleep hygiene are critical adjunctive behavioral therapies required to completely halt visceral fat accumulation.
The Context and Dangers of Anti-Obesity Pharmacotherapy
The recent pharmacological proliferation of highly potent anti-obesity medications, specifically Glucagon-Like Peptide-1 (GLP-1) receptor agonists, has radically altered the landscape of obesity management. While these powerful medications successfully drive massive, rapid fat loss and substantially improve markers of metabolic health, their clinical application requires intense, rigorous oversight regarding the patient’s underlying body composition.
During periods of rapid GLP-1-associated weight loss, clinical studies suggest that a startling 25%—and in certain highly catabolic cases, up to 40%—of the total weight lost can originate directly from the destruction of lean muscle mass and bone mineral density, rather than from targeted adipose tissue. For a patient presenting with Normal Weight Obesity, who is already teetering perilously on the edge of clinical sarcopenia and frailty, the unsupervised application of such pharmacotherapy without the simultaneous enforcement of a strict progressive resistance training program and a hyper-protein lifestyle protocol could prove metabolically catastrophic. In these scenarios, the medication may successfully eliminate the ectopic fat, but it will leave the patient in a state of worsened biological frailty, severe functional impairment, and permanent metabolic damage. Thus, the prescription of obesity pharmacotherapy must always be inextricably paired with lifestyle medicine focused directly on muscle preservation.
Conclusion
The traditional, global reliance on the simple anthropometric calculation of Body Mass Index to dictate the presence, absence, or severity of metabolic disease is an obsolete clinical paradigm that dangerously obscures the true extent of cardiometabolic dysfunction. Normal Weight Obesity—a complex pathophysiology driven by finite individual subcutaneous fat expandability, localized cellular lipotoxicity from diacylglycerols and ceramides, ectopic lipid deposition in the liver and visceral cavities, and the progressive, silent loss of skeletal muscle—represents a profound, underdiagnosed threat to global public health.
The necessary clinical transition to the Adiposity-Based Chronic Disease (ABCD) framework highlights the absolute necessity of complication-centric, personalized medical care, acknowledging that the anatomical location and endocrine behavior of adipose tissue are infinitely more critical to survival than its absolute macroscopic mass. By leveraging advanced diagnostic modalities such as Dual-Energy X-ray Absorptiometry (DEXA) and multi-frequency Bioelectrical Impedance Analysis (BIA), alongside highly pragmatic primary care markers like the waist-to-height ratio, clinicians can effectively identify at-risk metabolic phenotypes, particularly within genetically susceptible populations such as those of South Asian descent.
Clinical treatment protocols must permanently pivot away from archaic models demanding global weight reduction, and instead advance toward highly sophisticated, biologically targeted body recomposition strategies. Through aggressive, individualized interventions combining high-leucine dietary protein periodization, progressive mechanical resistance training, and structured aerobic cardiovascular conditioning, it is clinically possible to successfully reverse anabolic resistance, clear lipotoxic ectopic lipid stores, restore protective endocrine myokine signaling, and secure long-term metabolic homeostasis across all spans of age and body weight.